{"title":"Managing Nonagenarians with Acute Myocardial Infarction: Invasive versus Conservative Treatment.","authors":"Jooho Lee, Kyoung-Woo Seo, Jin-Sun Park, Hyoung-Mo Yang, Hong-Seok Lim, Byoung-Joo Choi, So-Yeon Choi, Myeong-Ho Yoon, Gyo-Seung Hwang, Seung-Jae Tahk, Joon-Han Shin","doi":"10.1155/2020/8885518","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Limited data are available to support an invasive treatment strategy in nonagenarians with acute myocardial infarction (AMI). We aimed to investigate whether percutaneous coronary intervention (PCI) is beneficial in this frail population.</p><p><strong>Methods: </strong>We retrospectively analyzed 41 nonagenarians with AMI (both ST-segment-elevation and non-ST-segment-elevation MI) between 2006 and 2015 in a single center. We assessed 30-day and one-year mortality rates according to the treatment strategy.</p><p><strong>Results: </strong>Among study subjects, 24 (59%) were treated with PCI (PCI group) and 17 (41%) were treated with conservative management (medical treatment group) per the clinician's discretion. The median follow-up duration was 30 months (0-74 months). Thirty-day mortality was lower in the PCI group than in the medical treatment group (17% vs. 65%; <i>P</i> < 0.001). One-year mortality was also lower in the PCI group than in the medical treatment group (21% vs. 76%; <i>P</i> < 0.001). The PCI group presented a 73% decreased risk of death (adjusted hazard ratio: 0.269; 95% confidence interval: 0.126-0.571; <i>P</i> < 0.001). In the Killip class 1 through 3 subgroups (<i>n</i> = 36), 30-day and one-year mortality were still higher among those in the medical treatment group (13% vs. 54% at 30 days; <i>P</i> < 0.001 and 17% vs. 69% at one year; <i>P</i> < 0.001). Landmark analysis after 30 days revealed no significant difference in the cumulative mortality rate between the two groups, indicating that the mortality difference was mainly determined within the first 30 days after AMI.</p><p><strong>Conclusion: </strong>Mortality after AMI was decreased in correlation with the invasive strategy relative to the conservative strategy, even in nonagenarians. Regardless of age, PCI should be considered in AMI patients. However, large-scale randomized controlled trials are needed to support our conclusion.</p>","PeriodicalId":9494,"journal":{"name":"Cardiology Research and Practice","volume":"2020 ","pages":"8885518"},"PeriodicalIF":1.8000,"publicationDate":"2020-11-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/8885518","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research and Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2020/8885518","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Limited data are available to support an invasive treatment strategy in nonagenarians with acute myocardial infarction (AMI). We aimed to investigate whether percutaneous coronary intervention (PCI) is beneficial in this frail population.
Methods: We retrospectively analyzed 41 nonagenarians with AMI (both ST-segment-elevation and non-ST-segment-elevation MI) between 2006 and 2015 in a single center. We assessed 30-day and one-year mortality rates according to the treatment strategy.
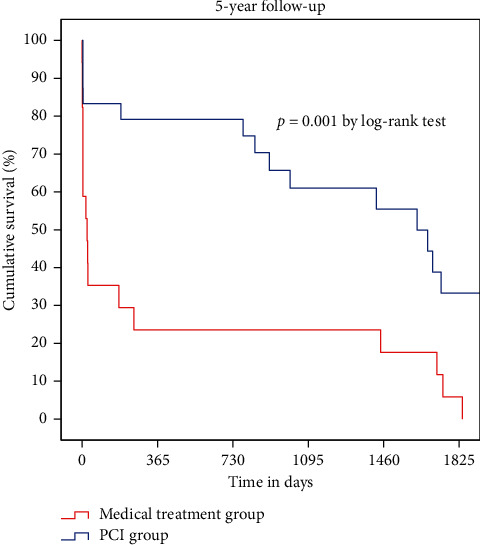
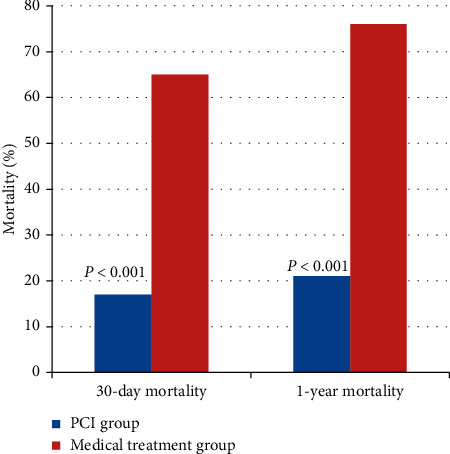
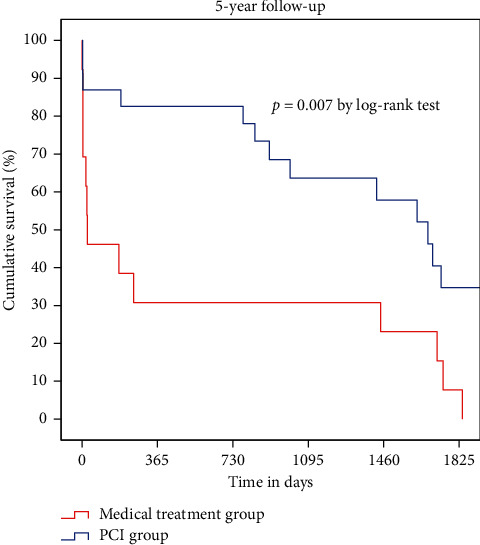
Results: Among study subjects, 24 (59%) were treated with PCI (PCI group) and 17 (41%) were treated with conservative management (medical treatment group) per the clinician's discretion. The median follow-up duration was 30 months (0-74 months). Thirty-day mortality was lower in the PCI group than in the medical treatment group (17% vs. 65%; P < 0.001). One-year mortality was also lower in the PCI group than in the medical treatment group (21% vs. 76%; P < 0.001). The PCI group presented a 73% decreased risk of death (adjusted hazard ratio: 0.269; 95% confidence interval: 0.126-0.571; P < 0.001). In the Killip class 1 through 3 subgroups (n = 36), 30-day and one-year mortality were still higher among those in the medical treatment group (13% vs. 54% at 30 days; P < 0.001 and 17% vs. 69% at one year; P < 0.001). Landmark analysis after 30 days revealed no significant difference in the cumulative mortality rate between the two groups, indicating that the mortality difference was mainly determined within the first 30 days after AMI.
Conclusion: Mortality after AMI was decreased in correlation with the invasive strategy relative to the conservative strategy, even in nonagenarians. Regardless of age, PCI should be considered in AMI patients. However, large-scale randomized controlled trials are needed to support our conclusion.
期刊介绍:
Cardiology Research and Practice is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies that focus on the diagnosis and treatment of cardiovascular disease. The journal welcomes submissions related to systemic hypertension, arrhythmia, congestive heart failure, valvular heart disease, vascular disease, congenital heart disease, and cardiomyopathy.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


