Dennis Kannenkeril, Shaun Frost, Janis M Nolde, Márcio Galindo Kiuchi, Revathy Carnagarin, Leslie Marisol Lugo-Gavidia, Justine Chan, Anu Joyson, Vance B Matthews, Lakshini Y Herat, Omar Azzam, Maryam Mehdizadeh, Janardhan Vignarajan, Yogesan Kanagasingam, Markus P Schlaich
{"title":"Microvascular changes at different stages of chronic kidney disease.","authors":"Dennis Kannenkeril, Shaun Frost, Janis M Nolde, Márcio Galindo Kiuchi, Revathy Carnagarin, Leslie Marisol Lugo-Gavidia, Justine Chan, Anu Joyson, Vance B Matthews, Lakshini Y Herat, Omar Azzam, Maryam Mehdizadeh, Janardhan Vignarajan, Yogesan Kanagasingam, Markus P Schlaich","doi":"10.1111/jch.14138","DOIUrl":null,"url":null,"abstract":"<p><p>Patients with progressing chronic kidney disease (CKD) are more likely to experience cardio- and cerebrovascular events than progressing to end-stage renal disease. The authors explored whether retinal microvascular calibers differed with the degree of renal impairment and between the standard and extended optic disk and may serve as a simple additional tool for risk stratification in this highly vulnerable patient cohort. The authors analyzed central retinal arteriolar and venular equivalent calibers (CRAE, CRVE) at different retinal zones (zone B&C) using digital retinal imaging in hypertensive patients with stage 2 (n = 66) or stage 3 CKD (n = 30). Results were adjusted for age, sex, HbA1c, and 24-hour diastolic blood pressure. Mean eGFR was 77.7 ± 8.9 and 48.8 ± 7.9 ml/min/1.73 m<sup>2</sup> for stage 2 and 3 CKD, respectively. CRAE and CRVE in zones B and C were significantly lower in patients with stage 3 CKD compared to patients with stage 2 CKD (CRAE-B:141.1 ± 21.4 vs. 130.5 ± 18.9 µm, p = .030; CRAE-C:137.4 ± 19.4 vs 129.2 ± 18.2 µm, p = .049; CRVE-B:220.8 ± 33.0 vs. 206.0 ± 28.4 µm, p = .004; and CRVE-C:215.9 ± 33.0 vs. 201.2 ± 25.1µm, p = .003). In patients with stage 2 CKD, CRAE-B was higher than CRAE-C (141.1 ± 21.4 vs. 137.4 ± 19.4µm, p < .001). In contrast, such a difference was not found in patients with stage 3 CKD. CRAE of both retinal zones correlated with eGFR for the entire cohort. In patients with stage 3 CKD, retinal narrowing is more pronounced compared to patients with stage 2 CKD. Whether the novel observation of difference in arteriolar caliber between zones B and C in stage 2 CKD could serve as an early marker of CKD progression warrants further investigation.</p>","PeriodicalId":520663,"journal":{"name":"Journal of clinical hypertension (Greenwich, Conn.)","volume":" ","pages":"309-316"},"PeriodicalIF":0.0000,"publicationDate":"2021-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1111/jch.14138","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical hypertension (Greenwich, Conn.)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/jch.14138","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/12/19 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 5
Abstract
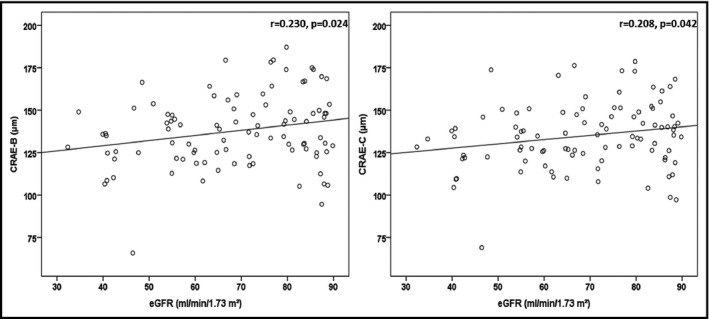
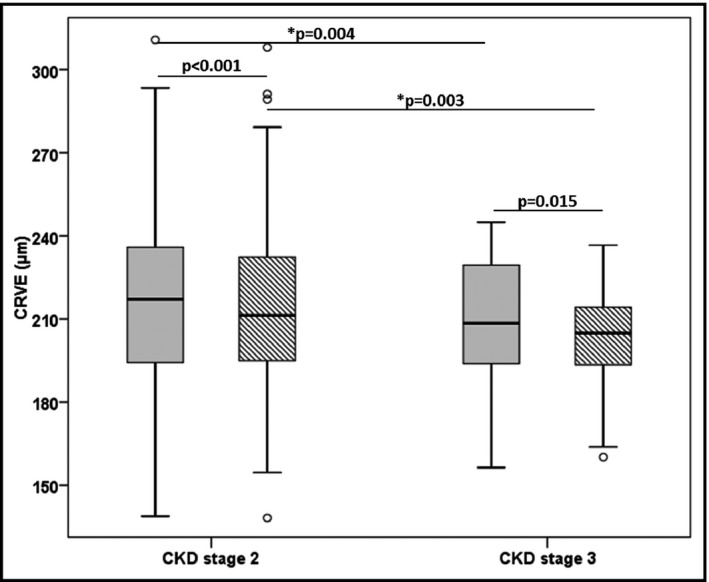
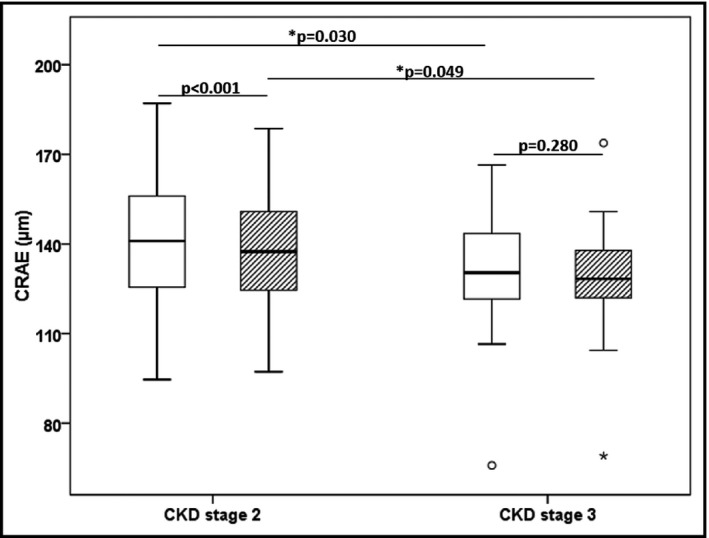
Patients with progressing chronic kidney disease (CKD) are more likely to experience cardio- and cerebrovascular events than progressing to end-stage renal disease. The authors explored whether retinal microvascular calibers differed with the degree of renal impairment and between the standard and extended optic disk and may serve as a simple additional tool for risk stratification in this highly vulnerable patient cohort. The authors analyzed central retinal arteriolar and venular equivalent calibers (CRAE, CRVE) at different retinal zones (zone B&C) using digital retinal imaging in hypertensive patients with stage 2 (n = 66) or stage 3 CKD (n = 30). Results were adjusted for age, sex, HbA1c, and 24-hour diastolic blood pressure. Mean eGFR was 77.7 ± 8.9 and 48.8 ± 7.9 ml/min/1.73 m2 for stage 2 and 3 CKD, respectively. CRAE and CRVE in zones B and C were significantly lower in patients with stage 3 CKD compared to patients with stage 2 CKD (CRAE-B:141.1 ± 21.4 vs. 130.5 ± 18.9 µm, p = .030; CRAE-C:137.4 ± 19.4 vs 129.2 ± 18.2 µm, p = .049; CRVE-B:220.8 ± 33.0 vs. 206.0 ± 28.4 µm, p = .004; and CRVE-C:215.9 ± 33.0 vs. 201.2 ± 25.1µm, p = .003). In patients with stage 2 CKD, CRAE-B was higher than CRAE-C (141.1 ± 21.4 vs. 137.4 ± 19.4µm, p < .001). In contrast, such a difference was not found in patients with stage 3 CKD. CRAE of both retinal zones correlated with eGFR for the entire cohort. In patients with stage 3 CKD, retinal narrowing is more pronounced compared to patients with stage 2 CKD. Whether the novel observation of difference in arteriolar caliber between zones B and C in stage 2 CKD could serve as an early marker of CKD progression warrants further investigation.
进展性慢性肾脏疾病(CKD)患者比进展为终末期肾脏疾病的患者更容易发生心脑血管事件。作者探讨了视网膜微血管直径是否随肾脏损害程度以及标准视盘和扩展视盘之间的差异而不同,并可作为这一高度易感患者队列中风险分层的简单附加工具。作者分析了2期(66例)或3期CKD(30例)高血压患者不同视网膜区(B&C区)中央视网膜小动脉和静脉等效口径(CRAE, CRVE)。结果根据年龄、性别、糖化血红蛋白和24小时舒张压进行了调整。2期和3期CKD的平均eGFR分别为77.7±8.9和48.8±7.9 ml/min/1.73 m2。3期CKD患者B区和C区CRAE和CRVE明显低于2期CKD患者(CRAE-B:141.1±21.4比130.5±18.9µm, p = 0.030;CRAE-C: 137.4±19.4 vs 129.2±18.2µm p = .049;CRVE-B: 220.8±33.0和206.0±28.4µm p = 04;和CRVE-C: 215.9±33.0和201.2±25.1µm p = .003)。在2期CKD患者中,CRAE-B高于CRAE-C(141.1±21.4 vs 137.4±19.4µm, p

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


