Denise Battaglini, Pasquale Anania, Patricia R M Rocco, Iole Brunetti, Alessandro Prior, Gianluigi Zona, Paolo Pelosi, Pietro Fiaschi
{"title":"Escalate and De-Escalate Therapies for Intracranial Pressure Control in Traumatic Brain Injury.","authors":"Denise Battaglini, Pasquale Anania, Patricia R M Rocco, Iole Brunetti, Alessandro Prior, Gianluigi Zona, Paolo Pelosi, Pietro Fiaschi","doi":"10.3389/fneur.2020.564751","DOIUrl":null,"url":null,"abstract":"<p><p>Severe traumatic brain injury (TBI) is frequently associated with an elevation of intracranial pressure (ICP), followed by cerebral perfusion pressure (CPP) reduction. Invasive monitoring of ICP is recommended to guide a step-by-step \"staircase approach\" which aims to normalize ICP values and reduce the risks of secondary damage. However, if such monitoring is not available clinical examination and radiological criteria should be used. A major concern is how to taper the therapies employed for ICP control. The aim of this manuscript is to review the criteria for escalating and withdrawing therapies in TBI patients. Each step of the staircase approach carries a risk of adverse effects related to the duration of treatment. Tapering of barbiturates should start once ICP control has been achieved for at least 24 h, although a period of 2-12 days is often required. Administration of hyperosmolar fluids should be avoided if ICP is normal. Sedation should be reduced after at least 24 h of controlled ICP to allow neurological examination. Removal of invasive ICP monitoring is suggested after 72 h of normal ICP. For patients who have undergone surgical decompression, cranioplasty represents the final step, and an earlier cranioplasty (15-90 days after decompression) seems to reduce the rate of infection, seizures, and hydrocephalus.</p>","PeriodicalId":2,"journal":{"name":"ACS Applied Bio Materials","volume":" ","pages":"564751"},"PeriodicalIF":4.6000,"publicationDate":"2020-11-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.3389/fneur.2020.564751","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Bio Materials","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fneur.2020.564751","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MATERIALS SCIENCE, BIOMATERIALS","Score":null,"Total":0}
引用次数: 7
Abstract
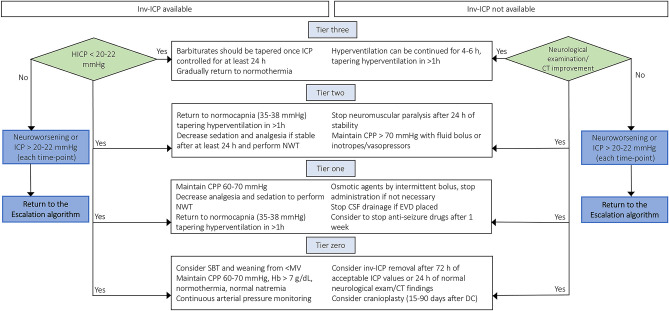
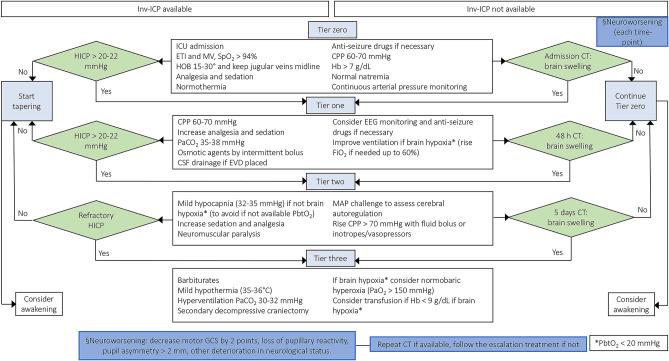
Severe traumatic brain injury (TBI) is frequently associated with an elevation of intracranial pressure (ICP), followed by cerebral perfusion pressure (CPP) reduction. Invasive monitoring of ICP is recommended to guide a step-by-step "staircase approach" which aims to normalize ICP values and reduce the risks of secondary damage. However, if such monitoring is not available clinical examination and radiological criteria should be used. A major concern is how to taper the therapies employed for ICP control. The aim of this manuscript is to review the criteria for escalating and withdrawing therapies in TBI patients. Each step of the staircase approach carries a risk of adverse effects related to the duration of treatment. Tapering of barbiturates should start once ICP control has been achieved for at least 24 h, although a period of 2-12 days is often required. Administration of hyperosmolar fluids should be avoided if ICP is normal. Sedation should be reduced after at least 24 h of controlled ICP to allow neurological examination. Removal of invasive ICP monitoring is suggested after 72 h of normal ICP. For patients who have undergone surgical decompression, cranioplasty represents the final step, and an earlier cranioplasty (15-90 days after decompression) seems to reduce the rate of infection, seizures, and hydrocephalus.
期刊介绍:
ACS Applied Bio Materials is an interdisciplinary journal publishing original research covering all aspects of biomaterials and biointerfaces including and beyond the traditional biosensing, biomedical and therapeutic applications.
The journal is devoted to reports of new and original experimental and theoretical research of an applied nature that integrates knowledge in the areas of materials, engineering, physics, bioscience, and chemistry into important bio applications. The journal is specifically interested in work that addresses the relationship between structure and function and assesses the stability and degradation of materials under relevant environmental and biological conditions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


