Dustin J Uhlenhopp, Oscar Aguilar, Dong Dai, Arka Ghosh, Michael Shaw, Chandan Mitra
{"title":"Hospital-Wide Medication Reconciliation Program: Error Identification, Cost-Effectiveness, and Detecting High-Risk Individuals on Admission.","authors":"Dustin J Uhlenhopp, Oscar Aguilar, Dong Dai, Arka Ghosh, Michael Shaw, Chandan Mitra","doi":"10.2147/IPRP.S269857","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Medication reconciliation (MR) on admission has potential to reduce negative patient outcomes. The objectives of this prospective observational study were to 1) measure the impact a hospital-wide MR program has on home medication error identification at hospital admission, 2) demonstrate cost-effectiveness of this program, and 3) identify risk factors placing individual patients at higher risk for medication discrepancies.</p><p><strong>Methods: </strong>Technicians obtained medication histories on adult patients admitted to the hospital that managed their own medications. Frequency and type of medication errors were recorded. Cost avoidance estimations were determined based on expected adverse drug event rates. Logistic regression analysis was used to test for associations between medication errors and patient characteristics. Results were considered significant when p-value was less than 0.05.</p><p><strong>Results: </strong>The study included 817 patients. Technicians recorded a mean of 6.1 medication discrepancies per patient (SD ± 0.4) and took 28.5 minutes (SD ± 1.2 minutes) to complete a medication history. Omission, commission, and dosing/frequency errors occurred in 82%, 59%, and 50% of medication histories, respectively. We estimated cost avoidance of $210.33 per patient with this program. Female gender, age, and high alert/risk medication use were linked to an increase in the likelihood of occurrence of a medication discrepancy.</p><p><strong>Conclusion: </strong>This study validated the ability of a pharmacy technician to identify errors, demonstrated economic cost-effectiveness, provided new data on time to obtain a BPMH, and further identified factors that contribute to the occurrence of medication discrepancies. Potentially harmful medication discrepancies were identified frequently on admission. With further research, it may be possible to identify those at highest risk for home medication discrepancies upon admission.</p>","PeriodicalId":45655,"journal":{"name":"Integrated Pharmacy Research and Practice","volume":"9 ","pages":"195-203"},"PeriodicalIF":2.1000,"publicationDate":"2020-10-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/IPRP.S269857","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Integrated Pharmacy Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/IPRP.S269857","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 7
Abstract
Background: Medication reconciliation (MR) on admission has potential to reduce negative patient outcomes. The objectives of this prospective observational study were to 1) measure the impact a hospital-wide MR program has on home medication error identification at hospital admission, 2) demonstrate cost-effectiveness of this program, and 3) identify risk factors placing individual patients at higher risk for medication discrepancies.
Methods: Technicians obtained medication histories on adult patients admitted to the hospital that managed their own medications. Frequency and type of medication errors were recorded. Cost avoidance estimations were determined based on expected adverse drug event rates. Logistic regression analysis was used to test for associations between medication errors and patient characteristics. Results were considered significant when p-value was less than 0.05.
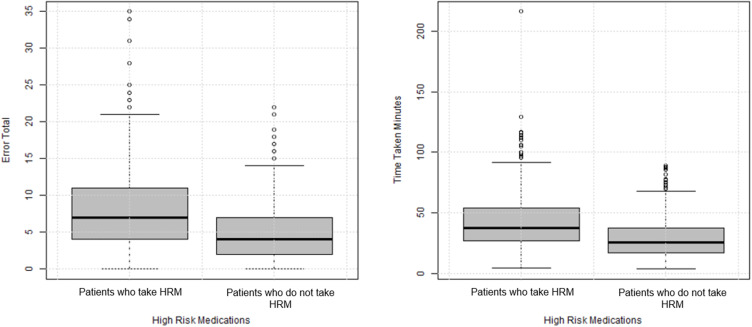
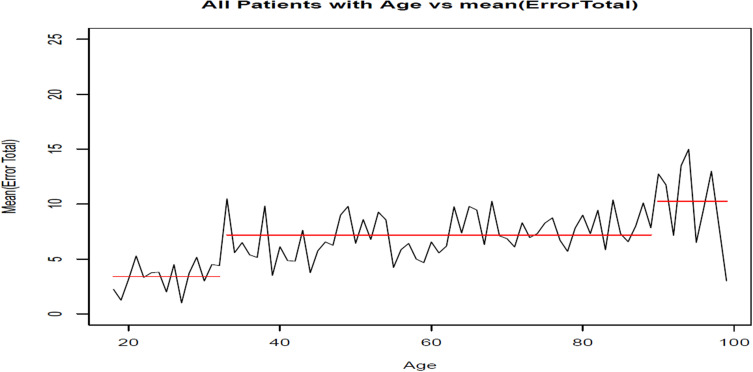
Results: The study included 817 patients. Technicians recorded a mean of 6.1 medication discrepancies per patient (SD ± 0.4) and took 28.5 minutes (SD ± 1.2 minutes) to complete a medication history. Omission, commission, and dosing/frequency errors occurred in 82%, 59%, and 50% of medication histories, respectively. We estimated cost avoidance of $210.33 per patient with this program. Female gender, age, and high alert/risk medication use were linked to an increase in the likelihood of occurrence of a medication discrepancy.
Conclusion: This study validated the ability of a pharmacy technician to identify errors, demonstrated economic cost-effectiveness, provided new data on time to obtain a BPMH, and further identified factors that contribute to the occurrence of medication discrepancies. Potentially harmful medication discrepancies were identified frequently on admission. With further research, it may be possible to identify those at highest risk for home medication discrepancies upon admission.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


