Barbara Bober, Marek Saracyn, Maciej Kołodziej, Łukasz Kowalski, Elżbieta Deptuła-Krawczyk, Waldemar Kapusta, Grzegorz Kamiński, Olga Mozenska, Jacek Bil
{"title":"Carcinoid Heart Disease: How to Diagnose and Treat in 2020?","authors":"Barbara Bober, Marek Saracyn, Maciej Kołodziej, Łukasz Kowalski, Elżbieta Deptuła-Krawczyk, Waldemar Kapusta, Grzegorz Kamiński, Olga Mozenska, Jacek Bil","doi":"10.1177/1179546820968101","DOIUrl":null,"url":null,"abstract":"<p><p>Neuroendocrine tumors (NETs, originally termed \"carcinoids\") create a relatively rare group of neoplasms with an approximate incidence rate of 2.5 to 5 cases per 100 000 persons. Roughly 30% to 40% of subjects with NETs develop carcinoid syndrome (CS), and 20% to 50% of subjects with CS are diagnosed with carcinoid heart disease (CaHD). The long-standing exposure to high serum serotonin concentration is one of the crucial factors in CaHD development. White plaque-like deposits on the endocardial surface of heart structures with valve leaflets and subvalvular apparatus thickening (fused and shortened chordae; thickened papillary muscles) are characteristic for CaHD. NT pro-BNP and 5-hydroxyindoleacetic acid are the 2 most useful screening markers. Long-acting somatostatin analogs are the standard of care in symptoms control. They are also the first-line treatment for tumor control in subjects with a metastatic somatostatin receptor avid disease. In cases refractory to somatostatin analogs, several options are available. We can increase a somatostatin analog to off-label doses, add telotristat ethyl or administer peptide receptor radionuclide therapy. Cardiac surgery, which mainly involves valve replacement, is presently the most efficient strategy in subjects with advanced CaHD and can relieve unmanageable symptoms or be partly responsible for better prognosis.</p>","PeriodicalId":10419,"journal":{"name":"Clinical Medicine Insights. Cardiology","volume":"14 ","pages":"1179546820968101"},"PeriodicalIF":2.3000,"publicationDate":"2020-10-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179546820968101","citationCount":"10","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179546820968101","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 10
Abstract
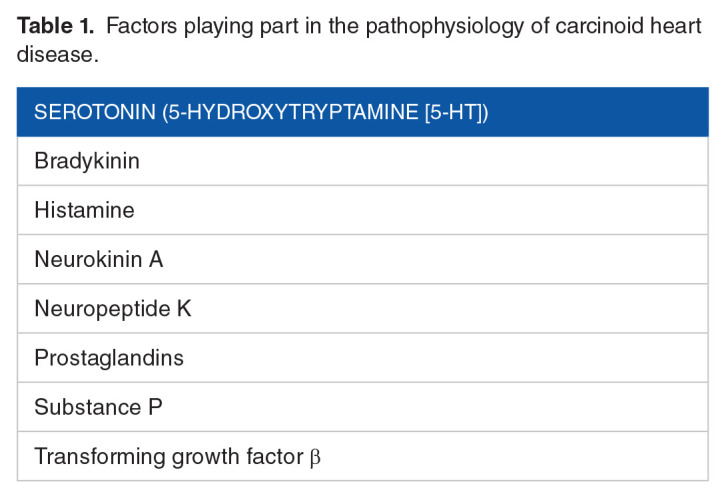
Neuroendocrine tumors (NETs, originally termed "carcinoids") create a relatively rare group of neoplasms with an approximate incidence rate of 2.5 to 5 cases per 100 000 persons. Roughly 30% to 40% of subjects with NETs develop carcinoid syndrome (CS), and 20% to 50% of subjects with CS are diagnosed with carcinoid heart disease (CaHD). The long-standing exposure to high serum serotonin concentration is one of the crucial factors in CaHD development. White plaque-like deposits on the endocardial surface of heart structures with valve leaflets and subvalvular apparatus thickening (fused and shortened chordae; thickened papillary muscles) are characteristic for CaHD. NT pro-BNP and 5-hydroxyindoleacetic acid are the 2 most useful screening markers. Long-acting somatostatin analogs are the standard of care in symptoms control. They are also the first-line treatment for tumor control in subjects with a metastatic somatostatin receptor avid disease. In cases refractory to somatostatin analogs, several options are available. We can increase a somatostatin analog to off-label doses, add telotristat ethyl or administer peptide receptor radionuclide therapy. Cardiac surgery, which mainly involves valve replacement, is presently the most efficient strategy in subjects with advanced CaHD and can relieve unmanageable symptoms or be partly responsible for better prognosis.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


