{"title":"Inter- and intra-core laboratory variability in the quantitative coronary angiography analysis for drug-eluting stent treatment and follow up.","authors":"Shigenori Ito, Kanako Kinoshita, Akiko Endo, Ryoko Kami, Yuko Kotake, Masato Nakamura","doi":"10.1177/1753944720958982","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To evaluate inter-core laboratory variability of quantitative coronary angiography (QCA) parameters in comparison with intra-core laboratory variability in a randomized controlled trial evaluating drug-eluting stents.</p><p><strong>Methods: </strong>A total of 50 patients with 62 coronary lesions were analyzed by four analysis experts belonging to an Angiographic Core Laboratory (ACL: 1 expert) and a Cardiovascular Imaging Core Laboratory (CICL: 3 experts). QCA was based on the same standard operating procedure, but selections of projection and cine frames were at the discretion of each analyst. Inter- and intra-core laboratory variabilities were evaluated by accuracy, precision, Bland Altman analysis, and coefficient of variation.</p><p><strong>Results: </strong>Pre-MLD (minimal lumen diameter) was significantly smaller in results from ACL than those from all CICL experts. Number of analyzed projections did not affect pre-MLD results. Acute gain was larger in ACL than in CICL2. No significant difference was observed in late loss and loss index between inter-core laboratories. Agreement between core labs in the Bland-Altman analysis for each QCA parameter was as follows (mean difference, 95% limits of agreement): pre-MLD (-0.32, -0.74 to 0.10), stent MLD (0.08, -0.28 to 0.44), acute gain (0.22, -0.44 to 0.88), and late loss (-0.07, -0.69 to 0.55). Agreement between analysts in CICL (mean difference, 95% limits of agreement) was: pre MLD (-0.03, -0.37 to 0.31), stent MLD (0.15, -0.15 to 0.45), acute gain (0.05, -0.45 to 0.55), and late loss (0.04, -0.52 to 0.60). The widest limits of agreement among three analyses were shown in both analyses. Width of limited agreement in the intra-core laboratory analysis tended to be smaller than the inter-core laboratory analysis with these parameters. Coefficient of variation tended to be larger in lesion length (LL), acute gain, late loss, and loss index in inter- and in intra- core laboratory comparisons.</p><p><strong>Conclusion: </strong>Inter-core laboratory QCA variability in late loss and loss index analysis could be similar to intra-core laboratory variability, but more strict alignment between core laboratories would be necessary for initial procedural data analysis.</p>","PeriodicalId":23035,"journal":{"name":"Therapeutic Advances in Cardiovascular Disease","volume":"14 ","pages":"1753944720958982"},"PeriodicalIF":2.2000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1a/a2/10.1177_1753944720958982.PMC7534069.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1753944720958982","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: To evaluate inter-core laboratory variability of quantitative coronary angiography (QCA) parameters in comparison with intra-core laboratory variability in a randomized controlled trial evaluating drug-eluting stents.
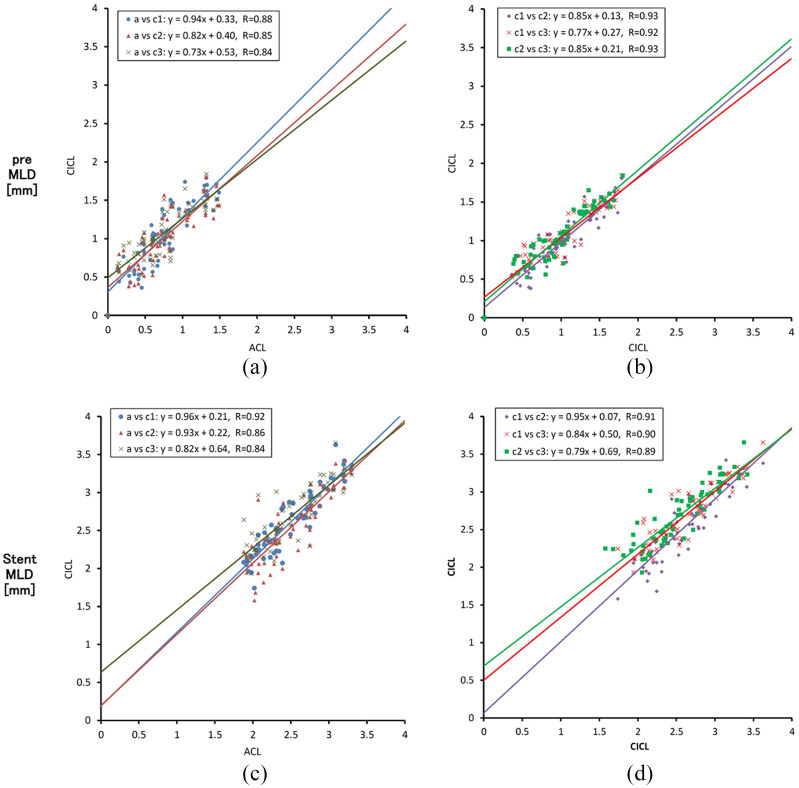
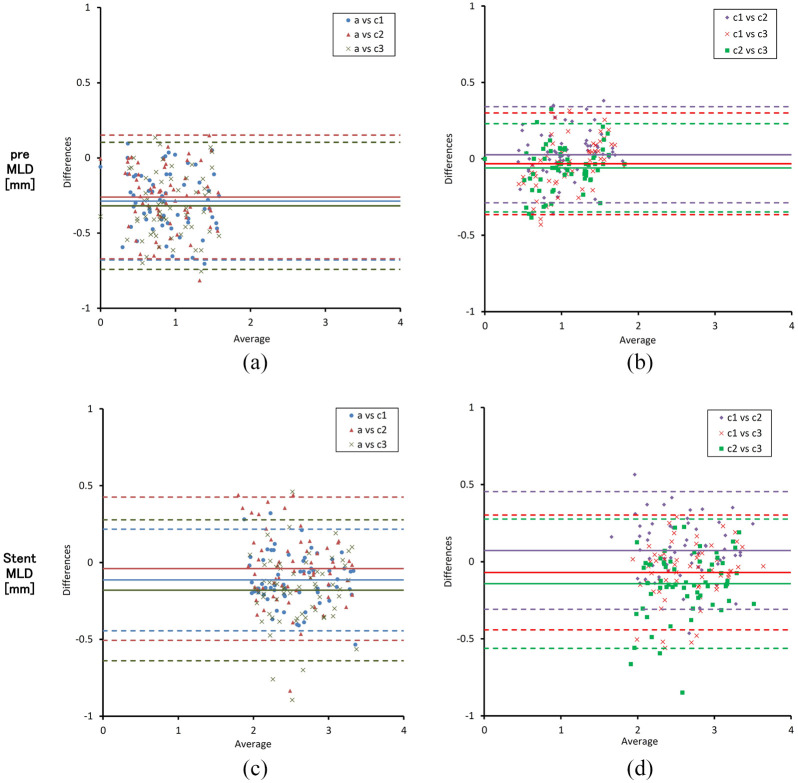
Methods: A total of 50 patients with 62 coronary lesions were analyzed by four analysis experts belonging to an Angiographic Core Laboratory (ACL: 1 expert) and a Cardiovascular Imaging Core Laboratory (CICL: 3 experts). QCA was based on the same standard operating procedure, but selections of projection and cine frames were at the discretion of each analyst. Inter- and intra-core laboratory variabilities were evaluated by accuracy, precision, Bland Altman analysis, and coefficient of variation.
Results: Pre-MLD (minimal lumen diameter) was significantly smaller in results from ACL than those from all CICL experts. Number of analyzed projections did not affect pre-MLD results. Acute gain was larger in ACL than in CICL2. No significant difference was observed in late loss and loss index between inter-core laboratories. Agreement between core labs in the Bland-Altman analysis for each QCA parameter was as follows (mean difference, 95% limits of agreement): pre-MLD (-0.32, -0.74 to 0.10), stent MLD (0.08, -0.28 to 0.44), acute gain (0.22, -0.44 to 0.88), and late loss (-0.07, -0.69 to 0.55). Agreement between analysts in CICL (mean difference, 95% limits of agreement) was: pre MLD (-0.03, -0.37 to 0.31), stent MLD (0.15, -0.15 to 0.45), acute gain (0.05, -0.45 to 0.55), and late loss (0.04, -0.52 to 0.60). The widest limits of agreement among three analyses were shown in both analyses. Width of limited agreement in the intra-core laboratory analysis tended to be smaller than the inter-core laboratory analysis with these parameters. Coefficient of variation tended to be larger in lesion length (LL), acute gain, late loss, and loss index in inter- and in intra- core laboratory comparisons.
Conclusion: Inter-core laboratory QCA variability in late loss and loss index analysis could be similar to intra-core laboratory variability, but more strict alignment between core laboratories would be necessary for initial procedural data analysis.
期刊介绍:
The journal is aimed at clinicians and researchers from the cardiovascular disease field and will be a forum for all views and reviews relating to this discipline.Topics covered will include: ·arteriosclerosis ·cardiomyopathies ·coronary artery disease ·diabetes ·heart failure ·hypertension ·metabolic syndrome ·obesity ·peripheral arterial disease ·stroke ·arrhythmias ·genetics


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


