Raman Sohal, Steven H Adams, Vishal Phogat, Abha Harish, Carlos Ynigo D Lopez, Michael P A Williams, Kamal K Khurana, Basel Abuzuaiter, Nia Jagroop, Bhavya Narapureddy
{"title":"Anti-NMDAR-Positive Small-Cell Lung Cancer Paraneoplastic Limbic Encephalitis: A Case Report and Literature Review.","authors":"Raman Sohal, Steven H Adams, Vishal Phogat, Abha Harish, Carlos Ynigo D Lopez, Michael P A Williams, Kamal K Khurana, Basel Abuzuaiter, Nia Jagroop, Bhavya Narapureddy","doi":"10.1155/2020/5269352","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Paraneoplastic limbic encephalitis (PLE) is a rare disease that presents as rapid onset dementia characterized by short-term memory loss (STM), anxiety, and behavioral changes. Anti-NMDAR antibodies are unfrequently reported in PLE associated with small-cell lung cancer (SCLC). Given that PLE can precede the diagnosis of cancer, it is very important that once infectious, metabolic, nutritional, or structural disorders associated with short-term memory loss are ruled out that vigorous effort must be made to rule out underlying malignancy.</p><p><strong>Case: </strong>We report a rare case of PLE as the presenting symptom of SCLC. A 72-year-old male with history of COPD was brought to the ED by his wife after he was found to have short-term memory loss, including forgetfulness of his wedding anniversary the day before, and anxiety. Neurological exam showed impaired short-term recall on MOCA. CT head showed no evidence of infarct. Lumbar puncture was performed which showed lymphocytic pleocytosis, a nonspecific inflammatory change. CSF panel was negative for HSV, <i>Neisseria</i>, <i>Hemophilus</i>, <i>E. coli</i>, and HIV. Initial EEG was unremarkable, though a repeat EEG showed mild slowing of the posterior dominant rhythm consistent with mild encephalopathy. MRI showed equivocal increased FLAIR on T2-weighted images in the bilateral temporal lobes, left greater than right. CTA thorax showed bulky mediastinal and right hilar LAD. FNA of the R4 lymph node revealed SCLC. The NM bone scan showed no osteoblastic lesions. While the serum autoantibody panel was positive for anti-NMDAR, the CSF autoantibody panel returned entirely negative. Chemotherapy with etoposide and cisplatin was started on Day 4 of admission. The patient's neurological symptoms showed improvement following chemotherapy.</p><p><strong>Conclusion: </strong>This case highlights the importance of recognizing short-term memory loss as a feature of PLE.</p>","PeriodicalId":9615,"journal":{"name":"Case Reports in Neurological Medicine","volume":"2020 ","pages":"5269352"},"PeriodicalIF":0.9000,"publicationDate":"2020-06-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/5269352","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Neurological Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/5269352","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Paraneoplastic limbic encephalitis (PLE) is a rare disease that presents as rapid onset dementia characterized by short-term memory loss (STM), anxiety, and behavioral changes. Anti-NMDAR antibodies are unfrequently reported in PLE associated with small-cell lung cancer (SCLC). Given that PLE can precede the diagnosis of cancer, it is very important that once infectious, metabolic, nutritional, or structural disorders associated with short-term memory loss are ruled out that vigorous effort must be made to rule out underlying malignancy.
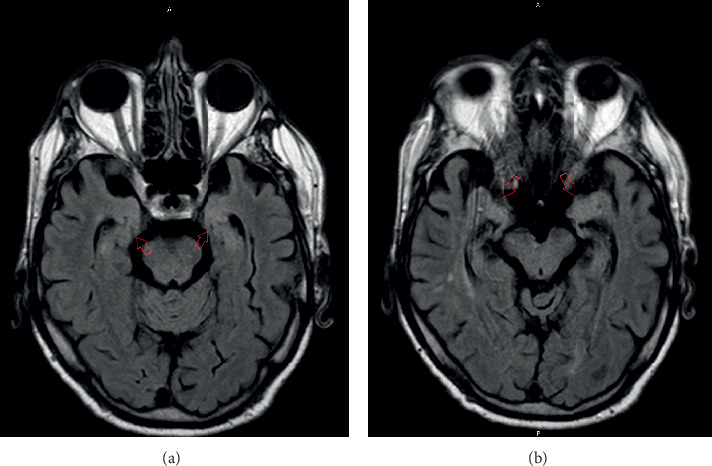
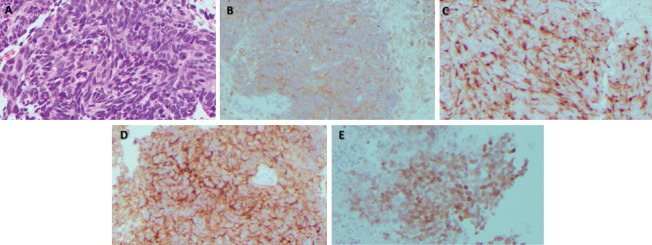
Case: We report a rare case of PLE as the presenting symptom of SCLC. A 72-year-old male with history of COPD was brought to the ED by his wife after he was found to have short-term memory loss, including forgetfulness of his wedding anniversary the day before, and anxiety. Neurological exam showed impaired short-term recall on MOCA. CT head showed no evidence of infarct. Lumbar puncture was performed which showed lymphocytic pleocytosis, a nonspecific inflammatory change. CSF panel was negative for HSV, Neisseria, Hemophilus, E. coli, and HIV. Initial EEG was unremarkable, though a repeat EEG showed mild slowing of the posterior dominant rhythm consistent with mild encephalopathy. MRI showed equivocal increased FLAIR on T2-weighted images in the bilateral temporal lobes, left greater than right. CTA thorax showed bulky mediastinal and right hilar LAD. FNA of the R4 lymph node revealed SCLC. The NM bone scan showed no osteoblastic lesions. While the serum autoantibody panel was positive for anti-NMDAR, the CSF autoantibody panel returned entirely negative. Chemotherapy with etoposide and cisplatin was started on Day 4 of admission. The patient's neurological symptoms showed improvement following chemotherapy.
Conclusion: This case highlights the importance of recognizing short-term memory loss as a feature of PLE.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


