{"title":"Acute Brainstem Dysfunction Caused by Cavernous Sinus Dural Arteriovenous Fistula.","authors":"Yuwa Oka, Kenichi Komatsu, Soichiro Abe, Naoya Yoshimoto, Junya Taki, Sadayuki Matsumoto","doi":"10.1155/2020/2630959","DOIUrl":null,"url":null,"abstract":"<p><p>Symptoms of cavernous sinus dural arteriovenous fistula depend on the drainage patterns and are very diverse. Among these, brainstem dysfunction is a rare but serious complication. Here, we describe a case with isolated and rapidly progressive brainstem dysfunction due to cavernous sinus dural arteriovenous fistula. An 80-year-old woman presented with a 2-day history of progressive gait disturbance. Neurological examination revealed mild confusion, dysarthria, and left hemiparesis. Magnetic resonance imaging (MRI) revealed pontine swelling without evidence of infarction. Magnetic resonance angiography suggested a faint abnormality near the cavernous sinus. Dural arteriovenous fistula was suspected, and digital subtraction angiography was planned for the next day. Her condition had progressed to coma by the next morning. Pontine swelling worsened, and hyperintensity appeared on diffusion-weighted imaging. Digital subtraction angiography revealed a right-sided cavernous sinus dural arteriovenous fistula with venous reflux into the posterior fossa. Orbital or ocular symptoms had preceded brainstem symptoms in all nine previously reported cases, but brainstem symptoms were the only presentation in our case, making the diagnosis difficult. Some dural arteriovenous fistulas mimic inflammatory diseases when the clinical course is acute. Prompt diagnosis using enhanced computed tomography or MRI and emergent treatment are needed to avoid permanent sequelae.</p>","PeriodicalId":9615,"journal":{"name":"Case Reports in Neurological Medicine","volume":"2020 ","pages":"2630959"},"PeriodicalIF":0.9000,"publicationDate":"2020-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7271059/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Neurological Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/2630959","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
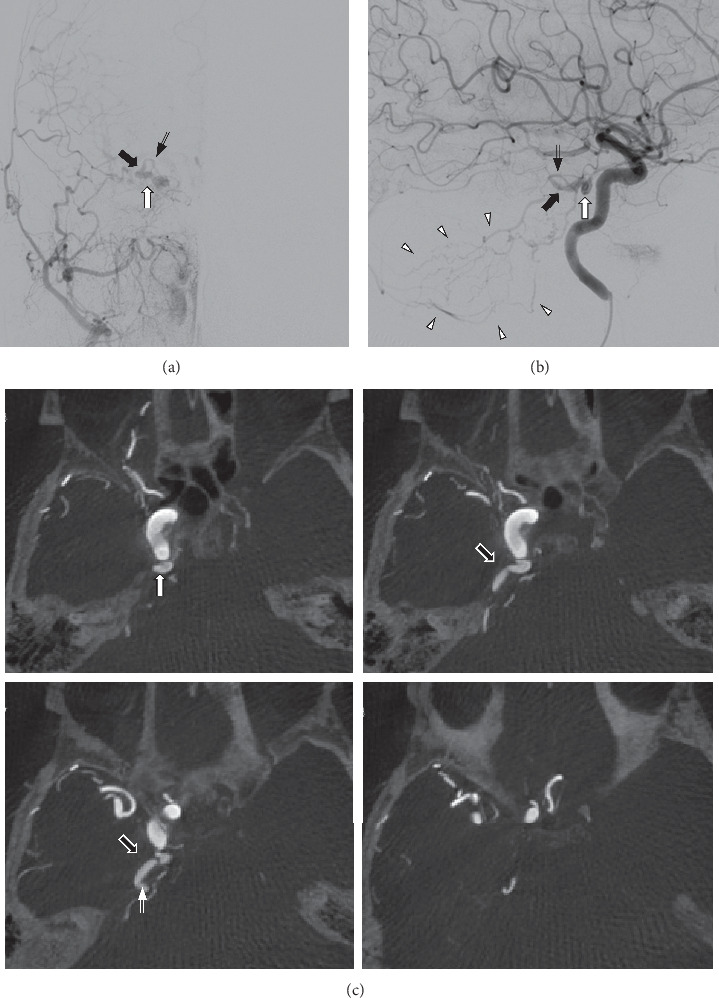
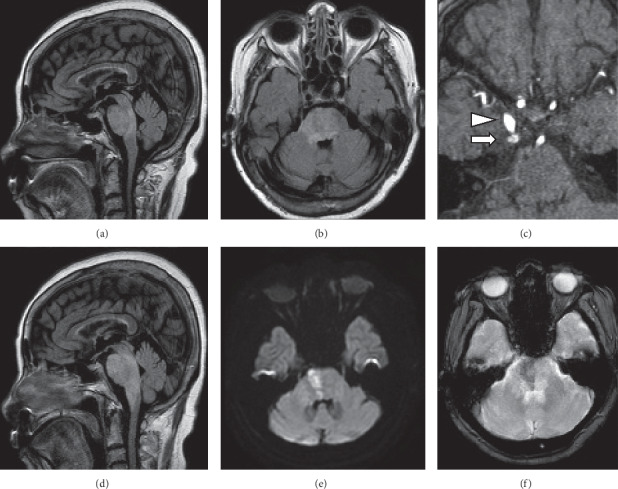
Symptoms of cavernous sinus dural arteriovenous fistula depend on the drainage patterns and are very diverse. Among these, brainstem dysfunction is a rare but serious complication. Here, we describe a case with isolated and rapidly progressive brainstem dysfunction due to cavernous sinus dural arteriovenous fistula. An 80-year-old woman presented with a 2-day history of progressive gait disturbance. Neurological examination revealed mild confusion, dysarthria, and left hemiparesis. Magnetic resonance imaging (MRI) revealed pontine swelling without evidence of infarction. Magnetic resonance angiography suggested a faint abnormality near the cavernous sinus. Dural arteriovenous fistula was suspected, and digital subtraction angiography was planned for the next day. Her condition had progressed to coma by the next morning. Pontine swelling worsened, and hyperintensity appeared on diffusion-weighted imaging. Digital subtraction angiography revealed a right-sided cavernous sinus dural arteriovenous fistula with venous reflux into the posterior fossa. Orbital or ocular symptoms had preceded brainstem symptoms in all nine previously reported cases, but brainstem symptoms were the only presentation in our case, making the diagnosis difficult. Some dural arteriovenous fistulas mimic inflammatory diseases when the clinical course is acute. Prompt diagnosis using enhanced computed tomography or MRI and emergent treatment are needed to avoid permanent sequelae.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


