{"title":"Posttraumatic Stress Disorder and Incident Type 2 Diabetes: Is Obesity to Blame?","authors":"Jeffrey F Scherrer, Patrick J Lustman","doi":"10.1177/2470547019863415","DOIUrl":null,"url":null,"abstract":"Numerous epidemiological studies have reported a positive association between posttraumatic stress disorder (PTSD) and higher risk for developing type 2 diabetes (T2D). Although several have shown that this association remains after controlling for measured confounding variables, few have discussed the large decrease in the magnitude of association after controlling for obesity, hyperlipidemia, hypertension, psychiatric conditions, and demographics. In a large cohort of Veterans Health Affairs (VHA) patients, results of age-adjusted Cox proportional hazard models indicated that patients with PTSD compared to those without were significantly more likely to develop T2D (hazard ratio1⁄4 1.33; 95% confidence interval: 1.08–1.64). After adjusting for obesity alone, the association was reduced by 50%. No statistical relationship remained after further adjustment for medical and psychiatric comorbidities. In this model, patients with obesity were 3.5 times more likely to develop T2D than those without, a finding that is consistent with the central role of obesity in the risk of T2D development. In fact, patients with obesity were equally likely to develop T2D (21/1000 Person Years [PY]) independent of PTSD. Likewise, in patients without obesity, the incident rate for T2D was 5.8/1000 PY and 6.4/1000 PY among patients with and without PTSD, respectively. So why do patients with PTSD and other common psychiatric disorders, for example, depression, have a higher risk for T2D compared to patients without these conditions? Their liability appears to rest largely on their propensity to become physically inactive, overweight, and obese. These factors are well-recognized risks in the population. Increasingly, it is recognized that medications (antidepressants and atypical antipsychotics) impose increases in weight and glucose dysregulation that add to risk of incident diabetes. The good news is that evidence has emerged demonstrating that lifestyle interventions work, lower significantly the risk of developing diabetes, and in persons with established diabetes, slow progression of diabetes. Interventions to address obesity are central to preventing cardiometabolic disease. Lifestyle interventions, that is, changes in dietary practices and moderate intensity (moderate intensity exercise >150min/week aimed at >5% weight loss) have proven efficacy. The Diabetes Prevention Trial showed that the intensive lifestyle interventions (metformin vs. placebo) was most effective at reducing weight and a 57% decrease in incident T2D. Longitudinal follow-up data from three large studies of lifestyle intervention for diabetes prevention indicate sustained reductions in risk for T2D: 45% reduction at 7 years in the Da Qing study, 43% reduction at 7 years in the Finnish Diabetes Prevention Study, and 27% reduction at 15 years in the US Diabetes Prevention Program outcomes Study. As a whole, this research clearly identify weight loss as the most powerful","PeriodicalId":52315,"journal":{"name":"Chronic Stress","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2019-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2470547019863415","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Stress","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2470547019863415","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/8/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Psychology","Score":null,"Total":0}
引用次数: 0
Abstract
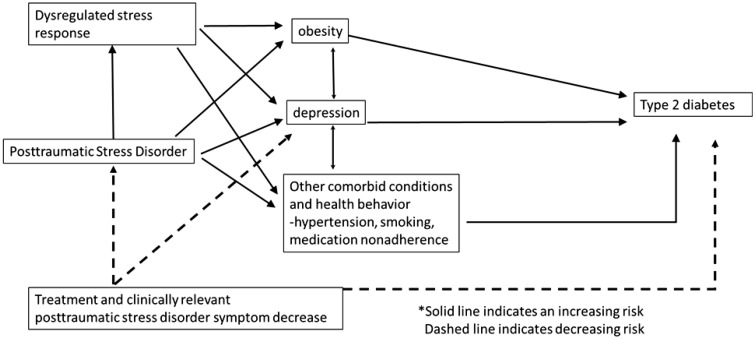
Numerous epidemiological studies have reported a positive association between posttraumatic stress disorder (PTSD) and higher risk for developing type 2 diabetes (T2D). Although several have shown that this association remains after controlling for measured confounding variables, few have discussed the large decrease in the magnitude of association after controlling for obesity, hyperlipidemia, hypertension, psychiatric conditions, and demographics. In a large cohort of Veterans Health Affairs (VHA) patients, results of age-adjusted Cox proportional hazard models indicated that patients with PTSD compared to those without were significantly more likely to develop T2D (hazard ratio1⁄4 1.33; 95% confidence interval: 1.08–1.64). After adjusting for obesity alone, the association was reduced by 50%. No statistical relationship remained after further adjustment for medical and psychiatric comorbidities. In this model, patients with obesity were 3.5 times more likely to develop T2D than those without, a finding that is consistent with the central role of obesity in the risk of T2D development. In fact, patients with obesity were equally likely to develop T2D (21/1000 Person Years [PY]) independent of PTSD. Likewise, in patients without obesity, the incident rate for T2D was 5.8/1000 PY and 6.4/1000 PY among patients with and without PTSD, respectively. So why do patients with PTSD and other common psychiatric disorders, for example, depression, have a higher risk for T2D compared to patients without these conditions? Their liability appears to rest largely on their propensity to become physically inactive, overweight, and obese. These factors are well-recognized risks in the population. Increasingly, it is recognized that medications (antidepressants and atypical antipsychotics) impose increases in weight and glucose dysregulation that add to risk of incident diabetes. The good news is that evidence has emerged demonstrating that lifestyle interventions work, lower significantly the risk of developing diabetes, and in persons with established diabetes, slow progression of diabetes. Interventions to address obesity are central to preventing cardiometabolic disease. Lifestyle interventions, that is, changes in dietary practices and moderate intensity (moderate intensity exercise >150min/week aimed at >5% weight loss) have proven efficacy. The Diabetes Prevention Trial showed that the intensive lifestyle interventions (metformin vs. placebo) was most effective at reducing weight and a 57% decrease in incident T2D. Longitudinal follow-up data from three large studies of lifestyle intervention for diabetes prevention indicate sustained reductions in risk for T2D: 45% reduction at 7 years in the Da Qing study, 43% reduction at 7 years in the Finnish Diabetes Prevention Study, and 27% reduction at 15 years in the US Diabetes Prevention Program outcomes Study. As a whole, this research clearly identify weight loss as the most powerful

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


