Matthew Wong-Pack, Nawazish Naqvi, George Ioannidis, Ramy Khalil, Alexandra Papaioannou, Jonathan Adachi, Arthur N Lau
{"title":"Evaluation of the Fracture Liaison Service within the Canadian Healthcare Setting.","authors":"Matthew Wong-Pack, Nawazish Naqvi, George Ioannidis, Ramy Khalil, Alexandra Papaioannou, Jonathan Adachi, Arthur N Lau","doi":"10.1155/2020/6742604","DOIUrl":null,"url":null,"abstract":"<p><p>Previous studies evaluating fracture liaison service (FLS) programs have found them to be cost-effective, efficient, and reduce the risk of fracture. However, few studies have evaluated the clinical effectiveness of these programs. We compared the patient populations of those referred for osteoporosis management by FLS to those referred by primary care physicians (PCP), within the Canadian healthcare system in the province of Ontario. Specifically, we investigated if a referral from FLS is similarly effective as PCP at identifying patients at risk for future osteoporotic fractures and if osteoporosis therapies have been previously initiated. A retrospective chart review of patients assessed by a single Ontario rheumatology practice affiliated with FLS between January 1, 2014, and December 31, 2017, was performed identifying two groups: those referred by FLS within Hamilton and those referred by their PCP for osteoporosis management. Fracture risk of each patient was determined using FRAX. A total of 573 patients (<i>n</i> = 225 (FLS group) and <i>n</i> = 227 (PCP group)) were evaluated. Between the FLS and PCP groups, there were no significant differences in the absolute 10-year risk of a major osteoporotic fracture (15.6% (SD = 10.2) vs 15.3% (SD = 10.3)) and 10-year risk of hip fracture (4.7% (SD = 8.3) vs 4.7% (SD = 6.8)), respectively. 10.7% of patients referred by FLS and 40.5% of patients referred by their PCP were on osteoporosis medication prior to fracture. Our study suggests that referral from FLS is similarly effective as PCP at identifying patients at risk for future osteoporotic fractures, and clinically effective at identifying the care gap with the previous use of targeted osteoporosis therapies from referral from PCP being low and much lower in those referred by FLS. Interventional programs such as FLS can help close the treatment gap by providing appropriate care to patients that were not previously identified to be at risk for fracture by their primary care physician and initiate proper medical management.</p>","PeriodicalId":45384,"journal":{"name":"Journal of Osteoporosis","volume":"2020 ","pages":"6742604"},"PeriodicalIF":3.0000,"publicationDate":"2020-03-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/6742604","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Osteoporosis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/6742604","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 2
Abstract
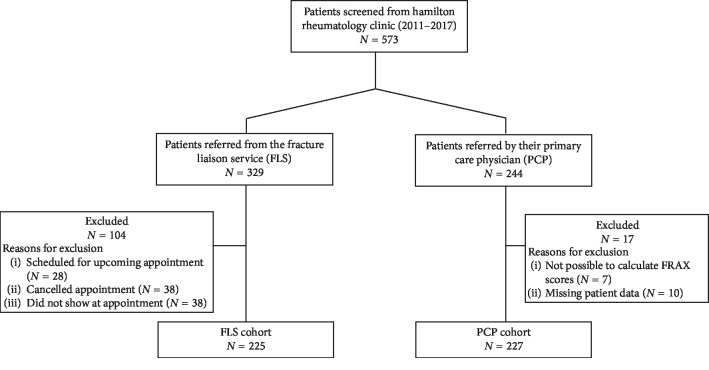
Previous studies evaluating fracture liaison service (FLS) programs have found them to be cost-effective, efficient, and reduce the risk of fracture. However, few studies have evaluated the clinical effectiveness of these programs. We compared the patient populations of those referred for osteoporosis management by FLS to those referred by primary care physicians (PCP), within the Canadian healthcare system in the province of Ontario. Specifically, we investigated if a referral from FLS is similarly effective as PCP at identifying patients at risk for future osteoporotic fractures and if osteoporosis therapies have been previously initiated. A retrospective chart review of patients assessed by a single Ontario rheumatology practice affiliated with FLS between January 1, 2014, and December 31, 2017, was performed identifying two groups: those referred by FLS within Hamilton and those referred by their PCP for osteoporosis management. Fracture risk of each patient was determined using FRAX. A total of 573 patients (n = 225 (FLS group) and n = 227 (PCP group)) were evaluated. Between the FLS and PCP groups, there were no significant differences in the absolute 10-year risk of a major osteoporotic fracture (15.6% (SD = 10.2) vs 15.3% (SD = 10.3)) and 10-year risk of hip fracture (4.7% (SD = 8.3) vs 4.7% (SD = 6.8)), respectively. 10.7% of patients referred by FLS and 40.5% of patients referred by their PCP were on osteoporosis medication prior to fracture. Our study suggests that referral from FLS is similarly effective as PCP at identifying patients at risk for future osteoporotic fractures, and clinically effective at identifying the care gap with the previous use of targeted osteoporosis therapies from referral from PCP being low and much lower in those referred by FLS. Interventional programs such as FLS can help close the treatment gap by providing appropriate care to patients that were not previously identified to be at risk for fracture by their primary care physician and initiate proper medical management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


