Mohammad K Choudhry, Bei Xiong, Antony Anandaraj, John Trillo
{"title":"Hepatic Cyst: An Unusual Suspect of Syncope.","authors":"Mohammad K Choudhry, Bei Xiong, Antony Anandaraj, John Trillo","doi":"10.1155/2020/1659718","DOIUrl":null,"url":null,"abstract":"<p><p>The patient is a 75-year-old man with history of diabetes and hypertension who presented with syncope after experiencing sharp, 10/10 right flank and abdominal pain worsening over three weeks associated with decreased appetite. Physical examination revealed hepatomegaly and right lower quadrant (RUQ) tenderness, negative for peritoneal signs. Bloodwork showed leukocytosis (13 K/mcl), alkaline phosphatase (141 U/L), total bilirubin (2.0 mg/dL), and gamma-glutamyl transferase (172 U/L). Computed Tomography (CT) revealed multiple hepatic cysts with the largest measuring 17 × 14 × 18 cm (Figure 1). Parenteral opiates provided minimal relief. Cardiac and neurologic etiologies of syncope were ruled out. The patient's course was complicated by opioid-induced delirium as his abdominal pain progressively worsened despite escalating doses of parenteral and oral analgesics. Gastroenterology and interventional radiology consulted to evaluate for Glisson's capsular stretch. Therapeutic aspiration yielded 2.5 L of serous fluid, which alleviated the patient's pain. Cytology was negative for malignancy. Opiates were titrated down. Repeat CT (Figure 2) showed cysts that were significantly reduced in size. The patient showed complete resolution of symptoms and was subsequently discharged. We present a rare case of a large hepatic cyst causing syncope. In the appropriate clinical setting, syncope with RUQ tenderness and hepatomegaly should raise the index of suspicion for hepatic cysts.</p>","PeriodicalId":30295,"journal":{"name":"Case Reports in Hepatology","volume":"2020 ","pages":"1659718"},"PeriodicalIF":0.0000,"publicationDate":"2020-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/1659718","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/1659718","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
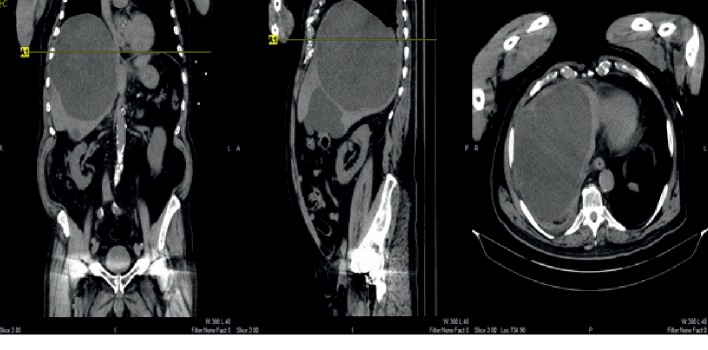
The patient is a 75-year-old man with history of diabetes and hypertension who presented with syncope after experiencing sharp, 10/10 right flank and abdominal pain worsening over three weeks associated with decreased appetite. Physical examination revealed hepatomegaly and right lower quadrant (RUQ) tenderness, negative for peritoneal signs. Bloodwork showed leukocytosis (13 K/mcl), alkaline phosphatase (141 U/L), total bilirubin (2.0 mg/dL), and gamma-glutamyl transferase (172 U/L). Computed Tomography (CT) revealed multiple hepatic cysts with the largest measuring 17 × 14 × 18 cm (Figure 1). Parenteral opiates provided minimal relief. Cardiac and neurologic etiologies of syncope were ruled out. The patient's course was complicated by opioid-induced delirium as his abdominal pain progressively worsened despite escalating doses of parenteral and oral analgesics. Gastroenterology and interventional radiology consulted to evaluate for Glisson's capsular stretch. Therapeutic aspiration yielded 2.5 L of serous fluid, which alleviated the patient's pain. Cytology was negative for malignancy. Opiates were titrated down. Repeat CT (Figure 2) showed cysts that were significantly reduced in size. The patient showed complete resolution of symptoms and was subsequently discharged. We present a rare case of a large hepatic cyst causing syncope. In the appropriate clinical setting, syncope with RUQ tenderness and hepatomegaly should raise the index of suspicion for hepatic cysts.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


