{"title":"Ultrasound-Guided Cervical Lymph Node Sampling Performed by Respiratory Physicians.","authors":"Mohammed Ahmed, Cyrus Daneshvar, David Breen","doi":"10.1159/000501119","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A variety of disease processes investigated by respiratory physicians can lead to cervical lymphadenopathy. Ultrasound (US) has revolutionised respiratory investigations, and neck ultrasound (NUS) is increasingly recognised as an additional important skill for respiratory physicians.</p><p><strong>Objectives: </strong>We aimed to assess the feasibility of NUS performed by respiratory physicians in the workup of patients with mediastinal lymphadenopathy.</p><p><strong>Methods: </strong>This is a single-centre retrospective cohort study. All patients that underwent US-guided cervical lymph node sampling were included. The diagnostic yield is reported, and specimen adequacy is compared for respiratory physicians and radiologists.</p><p><strong>Results: </strong>Over 5 years, 106 patients underwent NUS-guided lymph node sampling by respiratory physicians compared to 35 cases performed by radiologists. There was no significant difference in the adequacy of sampling between the two groups (respiratory physicians 91.5% [95% CI 84.5-96%] compared to 82.9% [95% CI 66.4-93.4%] for radiologists [<i>p</i> = 0.2]). In the respiratory physician group, a diagnosis was achieved based on lymph node sampling in 89 cases (84%). Neck lymph node sampling was the only procedure performed to obtain tissue in 48 cases (45.3%).</p><p><strong>Conclusion: </strong>NUS and sampling performed by respiratory physicians are feasible and associated with an adequacy rate comparable to that of radiologists. It can reduce the number of invasive procedures performed in a selected group of patients. Guidelines for training and competency assessment are required.</p>","PeriodicalId":9075,"journal":{"name":"Biomedicine Hub","volume":" ","pages":"1-6"},"PeriodicalIF":0.0000,"publicationDate":"2019-07-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000501119","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomedicine Hub","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000501119","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Background: A variety of disease processes investigated by respiratory physicians can lead to cervical lymphadenopathy. Ultrasound (US) has revolutionised respiratory investigations, and neck ultrasound (NUS) is increasingly recognised as an additional important skill for respiratory physicians.
Objectives: We aimed to assess the feasibility of NUS performed by respiratory physicians in the workup of patients with mediastinal lymphadenopathy.
Methods: This is a single-centre retrospective cohort study. All patients that underwent US-guided cervical lymph node sampling were included. The diagnostic yield is reported, and specimen adequacy is compared for respiratory physicians and radiologists.
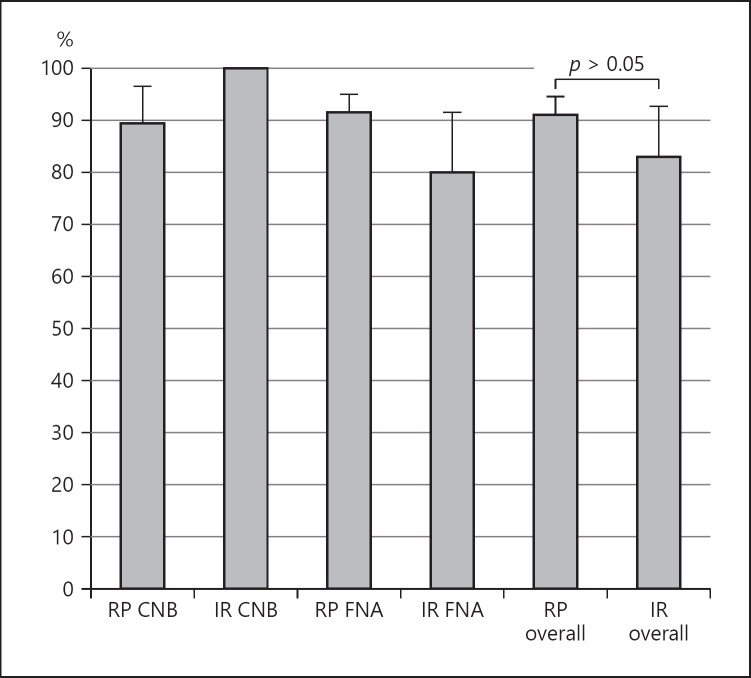
Results: Over 5 years, 106 patients underwent NUS-guided lymph node sampling by respiratory physicians compared to 35 cases performed by radiologists. There was no significant difference in the adequacy of sampling between the two groups (respiratory physicians 91.5% [95% CI 84.5-96%] compared to 82.9% [95% CI 66.4-93.4%] for radiologists [p = 0.2]). In the respiratory physician group, a diagnosis was achieved based on lymph node sampling in 89 cases (84%). Neck lymph node sampling was the only procedure performed to obtain tissue in 48 cases (45.3%).
Conclusion: NUS and sampling performed by respiratory physicians are feasible and associated with an adequacy rate comparable to that of radiologists. It can reduce the number of invasive procedures performed in a selected group of patients. Guidelines for training and competency assessment are required.
背景:呼吸内科医生研究的多种疾病过程可导致颈部淋巴结病。超声(US)已经彻底改变了呼吸检查,颈部超声(NUS)越来越被认为是呼吸内科医生的一项重要技能。目的:我们旨在评估呼吸内科医生在纵隔淋巴结病患者的检查中实施NUS的可行性。方法:这是一项单中心回顾性队列研究。所有接受us引导颈部淋巴结取样的患者均被纳入研究。报告了诊断率,并比较了呼吸内科医生和放射科医生的标本充分性。结果:在5年多的时间里,106例患者接受了由呼吸内科医生引导的淋巴结取样,而由放射科医生进行的只有35例。两组间抽样充分性无显著差异(呼吸内科医生91.5% [95% CI 84.5-96%],放射科医生82.9% [95% CI 66.4-93.4%] [p = 0.2])。在呼吸内科医生组,89例(84%)患者通过淋巴结取样获得诊断。颈部淋巴结取样是48例(45.3%)中唯一获得组织的程序。结论:由呼吸内科医生进行的NUS和抽样是可行的,其充分率与放射科医生相当。它可以减少在选定的一组患者中进行的侵入性手术的次数。培训和能力评估指南是必需的。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


