{"title":"Rapid Progression of Tracheoesophageal Fistula Caused by Immunotherapy Administered after Tracheal Stent Placement.","authors":"Shinjiro Mizuguchi, Makoto Takahama, Ryu Nakajima, Hidetoshi Inoue, Ryuichi Ito, Ryoji Yamamoto","doi":"10.1159/000501157","DOIUrl":null,"url":null,"abstract":"<p><p>Development of a tracheoesophageal fistula (TEF) is a serious complication of treatment for esophageal or lung cancer, especially following radiation therapy. However, development of a TEF as a complication of chemotherapy or tracheal stenting after surgical debulking is quite uncommon. We herein report a rare case involving a patient with advanced adenocarcinoma invading the mediastinum who rapidly developed a TEF after placement of a tracheal stent and administration of nivolumab immunotherapy. A 55-year-old heavy ex-smoker was diagnosed with lung adenocarcinoma with mediastinal invasion. Nine months after first-line therapy (chemotherapy and radiation therapy), he underwent treatment with nivolumab (3 mg/kg) as fourth-line therapy. Two weeks after the first dose, he underwent mechanical debulking of the tumor with tracheal stenting because of the rapid development of paraesophageal lymph node swelling and severe tracheal stenosis. He received a second dose of nivolumab 2 weeks later; however, imaging studies 12 days after this second dose revealed a huge fistula between the upper trachea and esophagus through a metastatic lymph node. Neither an additional stent nor replacement of the stent was considered because of the fistula site expansion and suffocation risk. Despite further treatment, the patient died of his primary disease 2 months later. Our findings will be of great interest to the readers, especially those involved in the clinical treatment of patients with advanced lung cancer treated by immunotherapy. The knowledge of potentially devastating TEF formation in the presence of transmural tracheal metastasis/invasion will allow clinicians to provide the best possible care for their patients.</p>","PeriodicalId":9075,"journal":{"name":"Biomedicine Hub","volume":" ","pages":"1-5"},"PeriodicalIF":0.0000,"publicationDate":"2019-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000501157","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomedicine Hub","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000501157","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
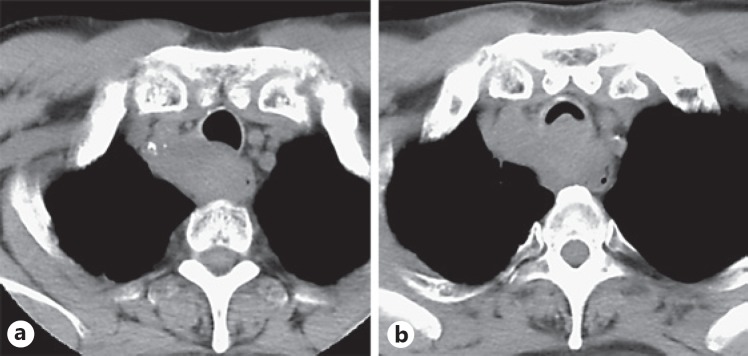
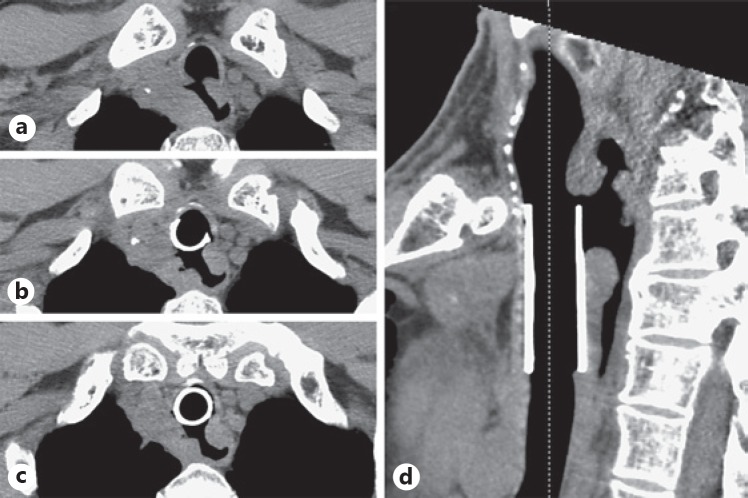
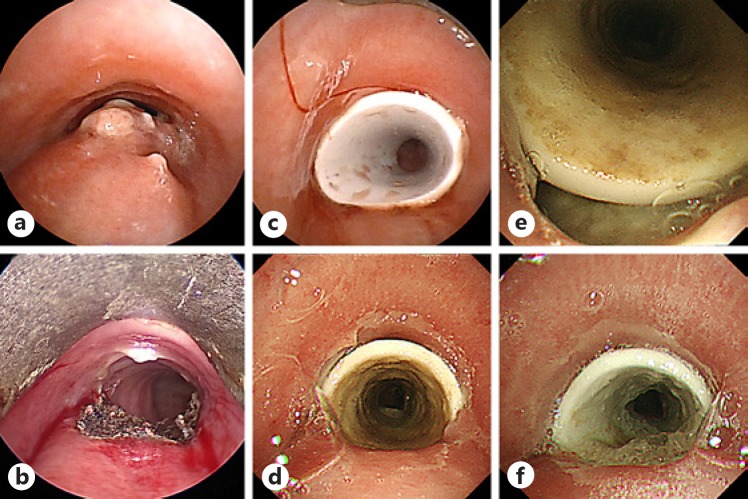
Development of a tracheoesophageal fistula (TEF) is a serious complication of treatment for esophageal or lung cancer, especially following radiation therapy. However, development of a TEF as a complication of chemotherapy or tracheal stenting after surgical debulking is quite uncommon. We herein report a rare case involving a patient with advanced adenocarcinoma invading the mediastinum who rapidly developed a TEF after placement of a tracheal stent and administration of nivolumab immunotherapy. A 55-year-old heavy ex-smoker was diagnosed with lung adenocarcinoma with mediastinal invasion. Nine months after first-line therapy (chemotherapy and radiation therapy), he underwent treatment with nivolumab (3 mg/kg) as fourth-line therapy. Two weeks after the first dose, he underwent mechanical debulking of the tumor with tracheal stenting because of the rapid development of paraesophageal lymph node swelling and severe tracheal stenosis. He received a second dose of nivolumab 2 weeks later; however, imaging studies 12 days after this second dose revealed a huge fistula between the upper trachea and esophagus through a metastatic lymph node. Neither an additional stent nor replacement of the stent was considered because of the fistula site expansion and suffocation risk. Despite further treatment, the patient died of his primary disease 2 months later. Our findings will be of great interest to the readers, especially those involved in the clinical treatment of patients with advanced lung cancer treated by immunotherapy. The knowledge of potentially devastating TEF formation in the presence of transmural tracheal metastasis/invasion will allow clinicians to provide the best possible care for their patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


