{"title":"Walking velocity and modified rivermead mobility index as discriminatory measures for functional ambulation classification of chronic stroke patients.","authors":"Ji Young Lim, Seung Heon An, Dae-Sung Park","doi":"10.1142/S1013702519500112","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The cut-off values of walking velocity and classification of functional mobility both have a role in clinical settings for assessing the walking function of stroke patients and setting rehabilitation goals and treatment plans.</p><p><strong>Objective: </strong>The present study investigated whether the cut-off values of the modified Rivermead Mobility Index (mRMI) and walking velocity accurately differentiated the walking ability of stroke patients according to the modified Functional Ambulation Category (mFAC).</p><p><strong>Methods: </strong>Eighty two chronic stroke patients were included in the study. The comfortable/maximum walking velocities and mRMI were used to measure the mobility outcomes of these patients. To compare the walking velocities and mRMI scores for each mFAC point, one-way analysis of variance and the post-hoc test using Scheffe's method were performed. The patients were categorized according to gait ability into either <math><mstyle><mtext>mFAC</mtext></mstyle> <mo>=</mo> <mstyle><mtext>VII</mtext></mstyle> </math> or mFAC <math><mo>≤</mo></math> VI group. The cut-off values for mRMI and walking velocities were calculated using a receiver-operating characteristic curve. The odds ratios of logistic regression analysis (Wald Forward) were analyzed to examine whether the cut-off values of walking velocity and mRMI can be utilized to differentiate functional walking levels.</p><p><strong>Results: </strong>Except for mFACs III and IV, maximum walking velocity differed between mFAC IV and mFAC V <math><mo>(</mo> <mi>p</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>01</mn> <mo>)</mo></math> , between mFAC V and mFAC VI <math><mo>(</mo> <mi>p</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>001</mn> <mo>)</mo></math> , and between mFAC VI and mFAC VII <math><mo>(</mo> <mi>p</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>05</mn> <mo>)</mo></math> . The cut-off value of mRMI is <math><mo>></mo> <mn>26</mn> <mo>.</mo> <mn>5</mn></math> and the area under the curve is 0.87, respectively; the cut-off value for comfortable walking velocity is <math><mo>></mo> <mn>0</mn> <mo>.</mo> <mn>77</mn></math> m/s and the area under the curve is 0.92, respectively; also, the cut-off value for maximum walking velocity is <math><mo>></mo> <mn>0</mn> <mo>.</mo> <mn>92</mn></math> m/s and the area under the curve is 0.97, respectively. In the logistic regression analysis, the maximum walking velocity <math><mo>(</mo> <mo>></mo> <mn>0</mn> <mo>.</mo> <mn>92</mn></math> m/s, <math><mstyle><mtext>OR</mtext></mstyle> <mo>=</mo> <mn>22</mn> <mo>.</mo> <mn>027</mn> <mo>)</mo></math> and mRMI <math><mo>(</mo> <mo>></mo> <mn>26</mn> <mo>.</mo> <mn>5</mn></math> scores, <math><mstyle><mtext>OR</mtext></mstyle> <mo>=</mo> <mn>10</mn> <mo>.</mo> <mn>283</mn> <mo>)</mo></math> are able to distinguish <math><mstyle><mtext>mFAC</mtext></mstyle> <mo>=</mo> <mstyle><mtext>VII</mtext></mstyle> </math> from mFAC <math><mo>≤</mo></math> VI.</p><p><strong>Conclusion: </strong>The cut-off values of maximum walking velocity and mRMI are recommended as useful outcome measures for assessing ambulation levels in chronic stroke patients during rehabilitation.</p>","PeriodicalId":44774,"journal":{"name":"Hong Kong Physiotherapy Journal","volume":"39 2","pages":"125-132"},"PeriodicalIF":1.0000,"publicationDate":"2019-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1142/S1013702519500112","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hong Kong Physiotherapy Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1142/S1013702519500112","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/5/21 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"REHABILITATION","Score":null,"Total":0}
引用次数: 5
Abstract
Background: The cut-off values of walking velocity and classification of functional mobility both have a role in clinical settings for assessing the walking function of stroke patients and setting rehabilitation goals and treatment plans.
Objective: The present study investigated whether the cut-off values of the modified Rivermead Mobility Index (mRMI) and walking velocity accurately differentiated the walking ability of stroke patients according to the modified Functional Ambulation Category (mFAC).
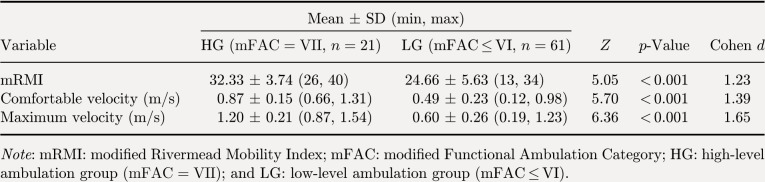
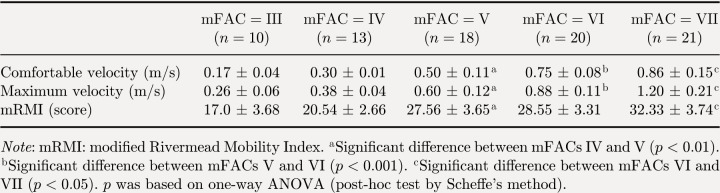
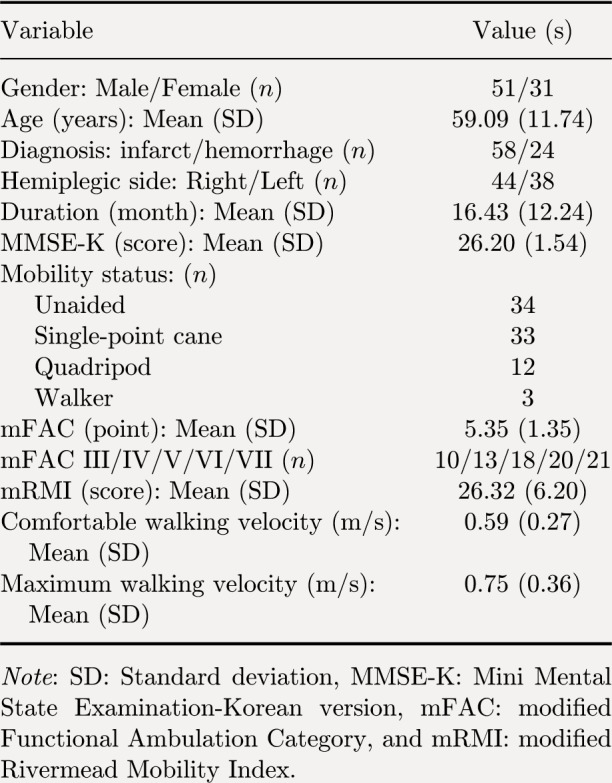
Methods: Eighty two chronic stroke patients were included in the study. The comfortable/maximum walking velocities and mRMI were used to measure the mobility outcomes of these patients. To compare the walking velocities and mRMI scores for each mFAC point, one-way analysis of variance and the post-hoc test using Scheffe's method were performed. The patients were categorized according to gait ability into either or mFAC VI group. The cut-off values for mRMI and walking velocities were calculated using a receiver-operating characteristic curve. The odds ratios of logistic regression analysis (Wald Forward) were analyzed to examine whether the cut-off values of walking velocity and mRMI can be utilized to differentiate functional walking levels.
Results: Except for mFACs III and IV, maximum walking velocity differed between mFAC IV and mFAC V , between mFAC V and mFAC VI , and between mFAC VI and mFAC VII . The cut-off value of mRMI is and the area under the curve is 0.87, respectively; the cut-off value for comfortable walking velocity is m/s and the area under the curve is 0.92, respectively; also, the cut-off value for maximum walking velocity is m/s and the area under the curve is 0.97, respectively. In the logistic regression analysis, the maximum walking velocity m/s, and mRMI scores, are able to distinguish from mFAC VI.
Conclusion: The cut-off values of maximum walking velocity and mRMI are recommended as useful outcome measures for assessing ambulation levels in chronic stroke patients during rehabilitation.
期刊介绍:
The Hong Kong Physiotherapy Journal is the official journal of the Hong Kong Physiotherapy Association Limited (HKPA Ltd). This peer-reviewed journal aims to contribute to and document the advancements in the principles and practice of physiotherapy in Hong Kong.The Hong Kong Physiotherapy Journal is published annually and papers are categorized into research reports, treatment reports, technical reports, literature reviews, and letters to the editor.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


