Religious and Psychosocial Covariates of Health-Related Quality of Life in People Living with HIV/AIDS.
HIV/AIDS research and treatment : open journal
Pub Date : 2015-02-01
Epub Date: 2015-02-10
DOI:10.17140/HARTOJ-1-101
引用次数: 18
Abstract
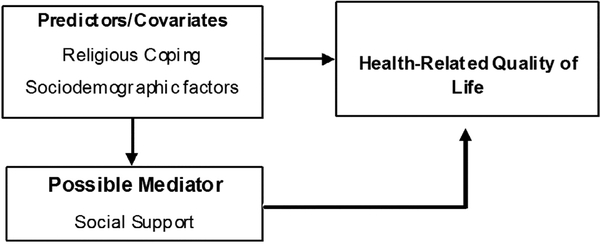
HIV/AIDS is a chronic, highly stigmatized illness that requires significant lifestyle adjustments, including consistent adherence to Antiretroviral Therapy (ART) in order for People Living With HIV/AIDS (PLWH) to survive and maintain good immune health. PLWH often report poor or moderate Health-Related Quality of Life (HRQoL) that is worse than the general population. This may be related to the psychological and physiological demands of HIV disease and the sociodemographic stressors associated with it. The role of religious coping, religiosity, and social support in the mental and physical dimensions of HRQoL is less known, although recent studies highlight that PLWH rely on spirituality/religion to cope with HIV-associated stressors. This study examined the effects of religious coping, religiosity, depressive symptoms, medication adherence, and social support satisfaction in various dimensions of Health- Related Quality of Life (HRQoL) in a sample of 292 PLWH. Majority of participants were African-American (90.1%) and 56.2% were male. Mean age was 45 years and, on average, participants lived with HIV for nearly 11 years. Descriptive statistics, correlations, Analysis of Variance (ANOVA), and hierarchical multiple linear regression were used to analyze the data. Income, sex (β= .14), age (β= −.14), depressive symptoms (β= −.27), and social support satisfaction (β= .17) significantly predicted physical HRQoL. Results indicate that income (β= .13), sex (β= .14), medication adherence (β= .13), negative religious coping (β= −.18), religious attendance (β= .13), religiousness (β= .16), and social support satisfaction (β= .27) significantly predicted mental HRQoL. Depressive symptoms (β= −.38), positive religious coping (β= .24), and social support satisfaction (β= .16) significantly predicted general HRQoL. Participants, who were female, prayed less than daily, attended religious services less than weekly or who were non/less religious had significantly poorer HRQoL. The findings confirm the importance of religion, mental health, medication adherence and social support in the HRQoL of PLWH, which should all be routinely assessed by clinicians.
艾滋病毒/艾滋病感染者健康相关生活质量的宗教和社会心理协变量
艾滋病毒/艾滋病是一种慢性、高度污名化的疾病,需要对生活方式进行重大调整,包括持续坚持抗逆转录病毒治疗(ART),以使艾滋病毒/艾滋病感染者(PLWH)生存并保持良好的免疫健康。PLWH经常报告较差或中等的健康相关生活质量(HRQoL),比一般人群更差。这可能与艾滋病毒疾病的心理和生理需求以及与之相关的社会人口压力因素有关。尽管最近的研究强调PLWH依靠灵性/宗教来应对hiv相关的压力源,但宗教应对、宗教信仰和社会支持在HRQoL的心理和身体维度中的作用尚不清楚。本研究以292名神职人员为样本,探讨宗教应对、宗教虔诚度、抑郁症状、药物依从性和社会支持满意度对健康相关生活质量(HRQoL)各维度的影响。大多数参与者是非裔美国人(90.1%),56.2%为男性。参与者的平均年龄为45岁,平均携带艾滋病毒近11年。采用描述性统计、相关性、方差分析(ANOVA)和层次多元线性回归分析数据。收入、性别(β= 0.14)、年龄(β= - 0.14)、抑郁症状(β= - 0.27)和社会支持满意度(β= 0.17)显著预测身体HRQoL。结果显示,收入(β= 0.13)、性别(β= 0.14)、药物依从性(β= 0.13)、消极宗教应对(β= - 0.18)、宗教出席(β= 0.13)、宗教虔诚(β= 0.16)、社会支持满意度(β= 0.27)与心理HRQoL有显著相关。抑郁症状(β= - 0.38)、积极的宗教应对(β= 0.24)和社会支持满意度(β= 0.16)显著预测总体HRQoL。女性、少于每天祈祷、少于每周参加宗教活动或不信教或不信教的参与者的HRQoL明显较差。研究结果证实了宗教信仰、心理健康、药物依从性和社会支持在PLWH的HRQoL中的重要性,这些都应该由临床医生进行常规评估。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


