Paul S Richman, Pomin Yeung, Thomas V Bilfinger, Jie Yang, William W Stringer
{"title":"Exercise Capacity in Unilateral Diaphragm Paralysis: The Effect of Obesity.","authors":"Paul S Richman, Pomin Yeung, Thomas V Bilfinger, Jie Yang, William W Stringer","doi":"10.1155/2019/1090982","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Healthy patients with unilateral diaphragm paralysis (UDP) are often asymptomatic; those with UDP and comorbidities that increase work of breathing are often dyspneic. We report the effect of obesity on exercise capacity in UDP patients.</p><p><strong>Methods: </strong>All obese and nonobese patients with UDP undergoing cardiopulmonary exercise testing (CPET) during a 32-month period in the exercise laboratory of an academic hospital were compared to a retrospectively identified cohort of obese and nonobese controls without UDP, matched for key features. CPET used a modified Bruce treadmill protocol with breath-to-breath expired gas analysis. O2 uptake, minute ventilation, exercise time, and work rate were recorded at peak exercise. Static pulmonary functions were measured. Kruskal-Wallis, Wilcoxon rank sum, and Fisher's exact tests were used to compare continuous and categorical variables, respectively. Stratified linear regression was used to quantify the effect of UDP and obesity on CPET variables.</p><p><strong>Results: </strong>Twenty-two UDP patients and 46 controls were studied. The BMI of obese and nonobese patients was 33.0±4.2 and 25.8±2.4 kg/m2, respectively. UDP subjects with obesity, compared to controls with neither condition, showed significantly reduced peak O2 uptake normalized to actual body weight (1.57±0.64 versus 2.01±0.88 L/min), shorter exercise time (5.7±2.0 versus 8.5±2.9 minutes), and lower peak ventilation. This was not observed in UDP alone or obesity alone. Peak work rate trended lower in the combined UDP-obesity group.</p><p><strong>Conclusion: </strong>Neither UDP nor obesity alone significantly reduced exercise capacity. Superimposed UDP and obesity interact to create a ventilatory limitation to exercise, with reduced peak-VO2, exercise time, and work rate.</p>","PeriodicalId":46434,"journal":{"name":"Pulmonary Medicine","volume":"2019 ","pages":"1090982"},"PeriodicalIF":2.1000,"publicationDate":"2019-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2019/1090982","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2019/1090982","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 4
Abstract
Purpose: Healthy patients with unilateral diaphragm paralysis (UDP) are often asymptomatic; those with UDP and comorbidities that increase work of breathing are often dyspneic. We report the effect of obesity on exercise capacity in UDP patients.
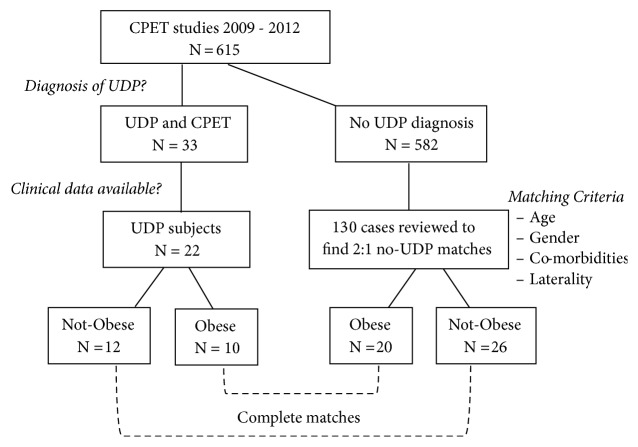
Methods: All obese and nonobese patients with UDP undergoing cardiopulmonary exercise testing (CPET) during a 32-month period in the exercise laboratory of an academic hospital were compared to a retrospectively identified cohort of obese and nonobese controls without UDP, matched for key features. CPET used a modified Bruce treadmill protocol with breath-to-breath expired gas analysis. O2 uptake, minute ventilation, exercise time, and work rate were recorded at peak exercise. Static pulmonary functions were measured. Kruskal-Wallis, Wilcoxon rank sum, and Fisher's exact tests were used to compare continuous and categorical variables, respectively. Stratified linear regression was used to quantify the effect of UDP and obesity on CPET variables.
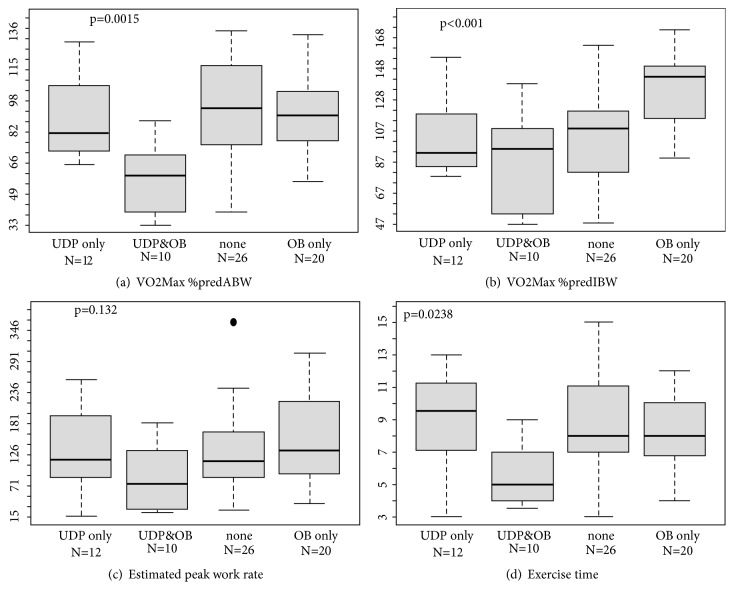
Results: Twenty-two UDP patients and 46 controls were studied. The BMI of obese and nonobese patients was 33.0±4.2 and 25.8±2.4 kg/m2, respectively. UDP subjects with obesity, compared to controls with neither condition, showed significantly reduced peak O2 uptake normalized to actual body weight (1.57±0.64 versus 2.01±0.88 L/min), shorter exercise time (5.7±2.0 versus 8.5±2.9 minutes), and lower peak ventilation. This was not observed in UDP alone or obesity alone. Peak work rate trended lower in the combined UDP-obesity group.
Conclusion: Neither UDP nor obesity alone significantly reduced exercise capacity. Superimposed UDP and obesity interact to create a ventilatory limitation to exercise, with reduced peak-VO2, exercise time, and work rate.
目的:健康的单侧膈肌麻痹(UDP)患者通常无症状;伴有UDP和增加呼吸工作量的合并症的患者常出现呼吸困难。我们报道肥胖对UDP患者运动能力的影响。方法:在一家学术医院的运动实验室进行了32个月的心肺运动试验(CPET),将所有肥胖和非肥胖的UDP患者与回顾性确定的无UDP的肥胖和非肥胖对照组进行了比较,主要特征匹配。CPET使用了改良的布鲁斯跑步机方案进行呼气呼气呼气分析。在运动高峰时记录氧气摄取、分钟通气量、运动时间和工作速率。测量静态肺功能。分别使用Kruskal-Wallis, Wilcoxon秩和和Fisher的精确检验来比较连续变量和分类变量。分层线性回归用于量化UDP和肥胖对CPET变量的影响。结果:研究了22例UDP患者和46例对照组。肥胖和非肥胖患者的BMI分别为33.0±4.2和25.8±2.4 kg/m2。与对照组相比,伴有肥胖的UDP受试者与实际体重相比,峰值氧摄取明显降低(1.57±0.64 L/min vs 2.01±0.88 L/min),运动时间缩短(5.7±2.0 min vs 8.5±2.9 min),通气峰值降低。这在UDP单独或肥胖单独中没有观察到。在udp -肥胖联合组中,峰值工作率呈下降趋势。结论:单纯UDP和肥胖均不能显著降低运动能力。叠加的UDP和肥胖相互作用,造成运动的通气限制,降低峰值vo2,运动时间和工作率。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


