Anomalous Innervation to the Extensor Digitorum Brevis.
IF 1
Q4 CLINICAL NEUROLOGY
Journal of Brachial Plexus and Peripheral Nerve Injury
Pub Date : 2019-05-02
eCollection Date: 2019-01-01
DOI:10.1055/s-0039-1685531
引用次数: 4
Abstract
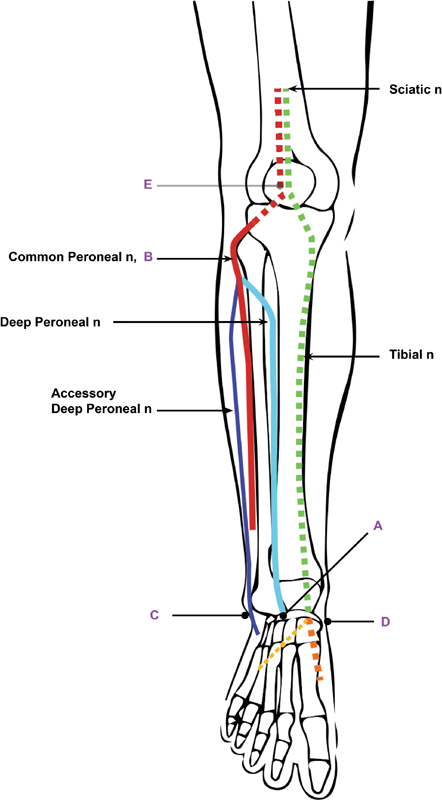
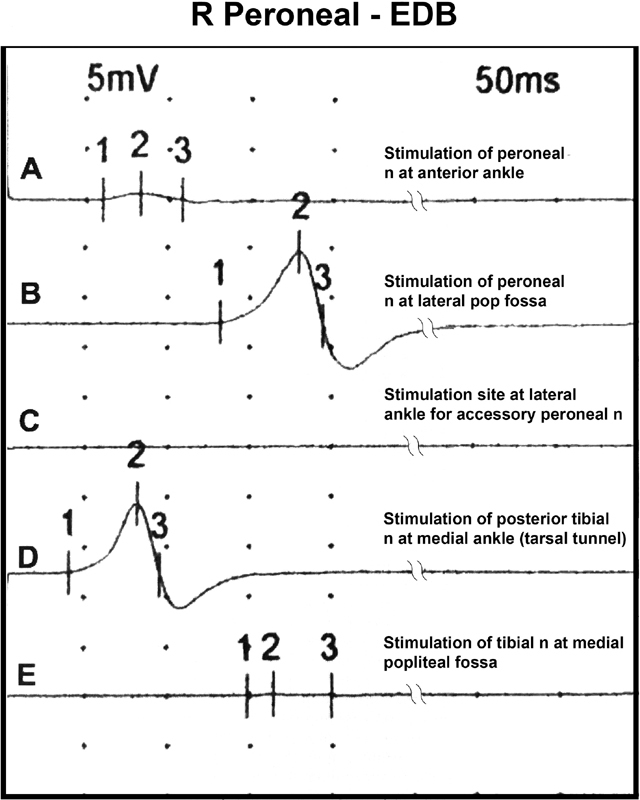
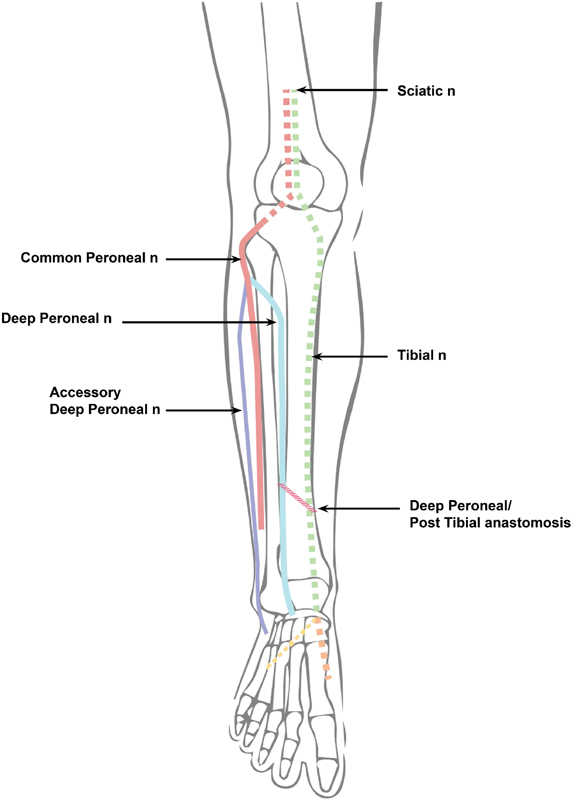
The nerve supply of the extensor digitorum brevis (EDB) usually arises from the deep peroneal nerve. An anomalous innervation arising from the accessory deep peroneal nerve is described in 15% of cases.1 An “all tibial foot” innervation pattern has been reported.2,3 In our clinic, electromyographic findings revealed the presence of a deep peroneal to posterior tibial nerve anastomosis similar to the forearm anastomosis of the median to ulnar nerve of Martin and Gruber. In ►Fig. 1, tracings of the EDB compound muscle action potential (CMAP) were generated after stimulation at various sites in the foreleg (►Fig. 2). The medially located tarsal tunnel is a site that will not generate an EDB CMAP unless there is an anomalous innervation to the EDB. In our cases, the distal peroneal site of stimulation failed to generate a maximal CMAP. Additional amplitude occurred after stimulation of the distal tibial nerve in the tarsal tunnel. Proximal peroneal and distal tibial nerve stimulations are characteristics of a cross over in the foreleg from the peroneal to the tibial nerve (►Fig. 3). Of 72 patients, 11% (8/72) showed these results. It was present in both legs in half of the patients (4/8). The finding of a deep peroneal to posterior tibial anastomosis will be of interest to neurologists performing electromyographic studies and surgeons that deal with injuries to the foreleg. In our sample, it wasmore frequent than the more widely known accessory deep peroneal variant. Fig. 1 Compound muscle action potential (CMAP) of the extensor digitorum brevis (EDB) stimulating from various points on the foreleg. Normally the amplitude of the CMAP of the EDB obtained by stimulation of the deep peroneal nerve at the ankle would be equal to that obtained by stimulation at the popliteal fossa, that is, trace A would equal with B. With a deep peroneal to posterior tibial anastomosis, a response is elicited by stimulating the posttibial nerve at the medial ankle (trace D). If there was an accessory deep peroneal nerve contribution, trace C would have a response. Proximal tibial stimulation would elicit a robust response in trace E in an “all tibial foot.”
指短伸肌神经支配异常。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Journal of Brachial Plexus and Peripheral Nerve Injury
CLINICAL NEUROLOGY-
CiteScore
1.70
自引率
14.30%
发文量
6
审稿时长
12 weeks
期刊介绍:
JBPPNI is an open access, peer-reviewed online journal that will encompass all aspects of basic and clinical research findings, in the area of brachial plexus and peripheral nerve injury. Injury in this context refers to congenital, inflammatory, traumatic, degenerative and neoplastic processes, including neurofibromatosis. Papers on diagnostic and imaging aspects of the peripheral nervous system are welcomed as well. The peripheral nervous system is unique in its complexity and scope of influence. There are areas of interest in the anatomy, physiology, metabolism, phylogeny, and limb growth tropism of peripheral nerves.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


