Uttara Partap, Elizabeth H Young, Pascale Allotey, Manjinder S Sandhu, Daniel D Reidpath
{"title":"Characterisation and correlates of stunting among Malaysian children and adolescents aged 6-19 years.","authors":"Uttara Partap, Elizabeth H Young, Pascale Allotey, Manjinder S Sandhu, Daniel D Reidpath","doi":"10.1017/gheg.2019.1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite emerging evidence regarding the reversibility of stunting at older ages, most stunting research continues to focus on children below 5 years of age. We aimed to assess stunting prevalence and examine the sociodemographic distribution of stunting risk among older children and adolescents in a Malaysian population.</p><p><strong>Methods: </strong>We used cross-sectional data on 6759 children and adolescents aged 6-19 years living in Segamat, Malaysia. We compared prevalence estimates for stunting defined using the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) references, using Cohen's <i>κ</i> coefficient. Associations between sociodemographic indices and stunting risk were examined using mixed-effects Poisson regression with robust standard errors.</p><p><strong>Results: </strong>The classification of children and adolescents as stunted or normal height differed considerably between the two references (CDC <i>v</i>. WHO; <i>κ</i> for agreement: 0.73), but prevalence of stunting was high regardless of reference (crude prevalence: CDC 29.2%; WHO: 19.1%). Stunting risk was approximately 19% higher among underweight <i>v</i>. normal weight children and adolescents (<i>p</i> = 0.030) and 21% lower among overweight children and adolescents (<i>p</i> = 0.001), and decreased strongly with improved household drinking water sources [risk ratio (RR) for water piped into house: 0.35, 95% confidence interval (95% CI) 0.30-0.41, <i>p</i> < 0.001). Protective effects were also observed for improved sanitation facilities (RR for flush toilet: 0.41, 95% CI 0.19-0.88, <i>p</i> = 0.023). Associations were not materially affected in multiple sensitivity analyses.</p><p><strong>Conclusions: </strong>Our findings justify a framework for strategies addressing stunting across childhood, and highlight the need for consensus on a single definition of stunting in older children and adolescents to streamline monitoring efforts.</p>","PeriodicalId":44052,"journal":{"name":"Global Health Epidemiology and Genomics","volume":"4 ","pages":"e2"},"PeriodicalIF":1.1000,"publicationDate":"2019-03-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6415126/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Health Epidemiology and Genomics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1017/gheg.2019.1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Despite emerging evidence regarding the reversibility of stunting at older ages, most stunting research continues to focus on children below 5 years of age. We aimed to assess stunting prevalence and examine the sociodemographic distribution of stunting risk among older children and adolescents in a Malaysian population.
Methods: We used cross-sectional data on 6759 children and adolescents aged 6-19 years living in Segamat, Malaysia. We compared prevalence estimates for stunting defined using the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) references, using Cohen's κ coefficient. Associations between sociodemographic indices and stunting risk were examined using mixed-effects Poisson regression with robust standard errors.
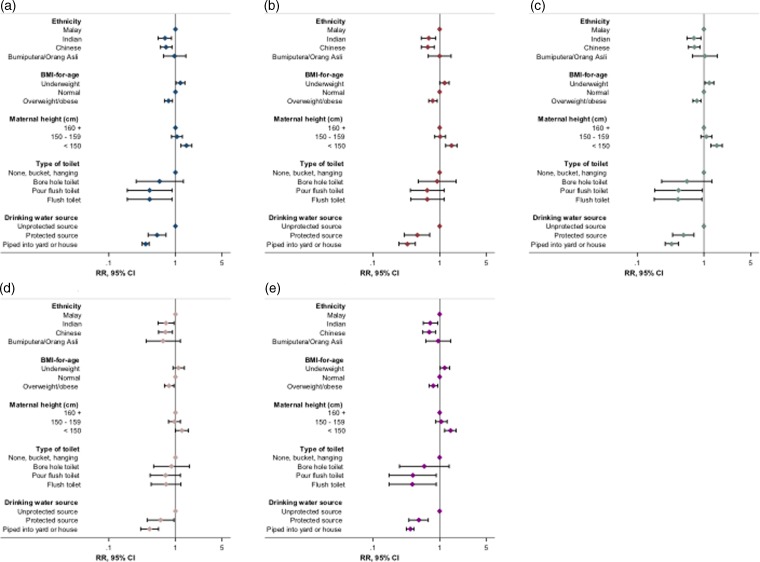
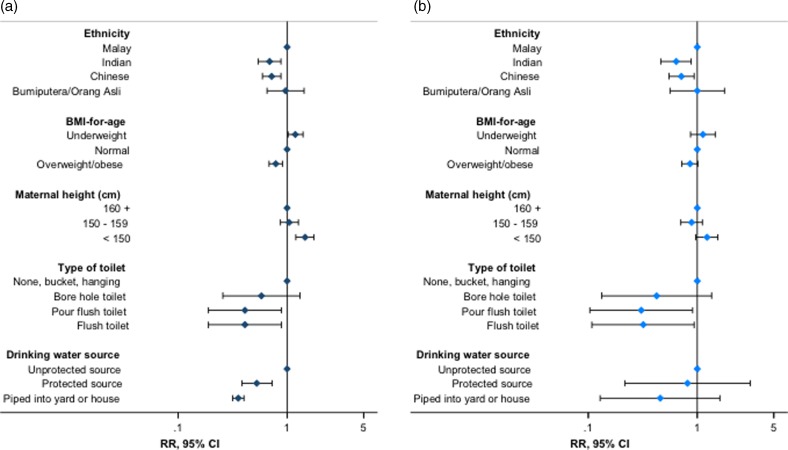
Results: The classification of children and adolescents as stunted or normal height differed considerably between the two references (CDC v. WHO; κ for agreement: 0.73), but prevalence of stunting was high regardless of reference (crude prevalence: CDC 29.2%; WHO: 19.1%). Stunting risk was approximately 19% higher among underweight v. normal weight children and adolescents (p = 0.030) and 21% lower among overweight children and adolescents (p = 0.001), and decreased strongly with improved household drinking water sources [risk ratio (RR) for water piped into house: 0.35, 95% confidence interval (95% CI) 0.30-0.41, p < 0.001). Protective effects were also observed for improved sanitation facilities (RR for flush toilet: 0.41, 95% CI 0.19-0.88, p = 0.023). Associations were not materially affected in multiple sensitivity analyses.
Conclusions: Our findings justify a framework for strategies addressing stunting across childhood, and highlight the need for consensus on a single definition of stunting in older children and adolescents to streamline monitoring efforts.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


