Comparison of Diaphragmatic Stretch Technique and Manual Diaphragm Release Technique on Diaphragmatic Excursion in Chronic Obstructive Pulmonary Disease: A Randomized Crossover Trial.
{"title":"Comparison of Diaphragmatic Stretch Technique and Manual Diaphragm Release Technique on Diaphragmatic Excursion in Chronic Obstructive Pulmonary Disease: A Randomized Crossover Trial.","authors":"Aishwarya Nair, Gopala Krishna Alaparthi, Shyam Krishnan, Santhosh Rai, R Anand, Vishak Acharya, Preetam Acharya","doi":"10.1155/2019/6364376","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic Obstructive Pulmonary Disease (COPD) impairs the function of the diaphragm by placing it at a mechanical disadvantage, shortening its operating length and changing the mechanical linkage between its various parts. This makes the diaphragm's contraction less effective in raising and expanding the lower rib cage, thereby increasing the work of breathing and reducing the functional capacity.</p><p><strong>Aim of the study: </strong>To compare the effects of diaphragmatic stretch and manual diaphragm release technique on diaphragmatic excursion in patients with COPD.</p><p><strong>Materials and methods: </strong>This randomised crossover trial included 20 clinically stable patients with mild and moderate COPD classified according to the GOLD criteria. The patients were allocated to group A or group B by block randomization done by primary investigator. The information about the technique was concealed in a sealed opaque envelope and revealed to the patients only after allocation of groups. After taking the demographic data and baseline values of the outcome measures (diaphragm mobility by ultrasonography performed by an experienced radiologist and chest expansion by inch tape performed by the therapist), group A subjects underwent the diaphragmatic stretch technique and the group B subjects underwent the manual diaphragm release technique. Both the interventions were performed in 2 sets of 10 deep breaths with 1-minute interval between the sets. The two outcome variables were recorded immediately after the intervention. A wash-out period of 3 hours was maintained to neutralize the effect of given intervention. Later the patients of group A and group B were crossed over to the other group.</p><p><strong>Results: </strong>In the diaphragmatic stretch technique, there was a statistically significant improvement in the diaphragmatic excursion before and after the treatment. On the right side, p=0.00 and p=0.003 in the midclavicular line and midaxillary line. On the left side, p=0.004 and p=0.312 in the midclavicular and midaxillary line. In manual diaphragm release technique, there was a statistically significant improvement before and after the treatment. On the right side, p=0.000 and p=0.000 in the midclavicular line and midaxillary line. On the left side, p=0.002 and p=0.000 in the midclavicular line and midaxillary line. There was no statistically significant difference in diaphragmatic excursion in the comparison of the postintervention values of both techniques.</p><p><strong>Conclusion: </strong>The diaphragmatic stretch technique and manual diaphragm release technique can be safely recommended for patients with clinically stable COPD to improve diaphragmatic excursion.</p>","PeriodicalId":46434,"journal":{"name":"Pulmonary Medicine","volume":"2019 ","pages":"6364376"},"PeriodicalIF":2.0000,"publicationDate":"2019-01-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2019/6364376","citationCount":"27","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2019/6364376","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 27
Abstract
Background: Chronic Obstructive Pulmonary Disease (COPD) impairs the function of the diaphragm by placing it at a mechanical disadvantage, shortening its operating length and changing the mechanical linkage between its various parts. This makes the diaphragm's contraction less effective in raising and expanding the lower rib cage, thereby increasing the work of breathing and reducing the functional capacity.
Aim of the study: To compare the effects of diaphragmatic stretch and manual diaphragm release technique on diaphragmatic excursion in patients with COPD.
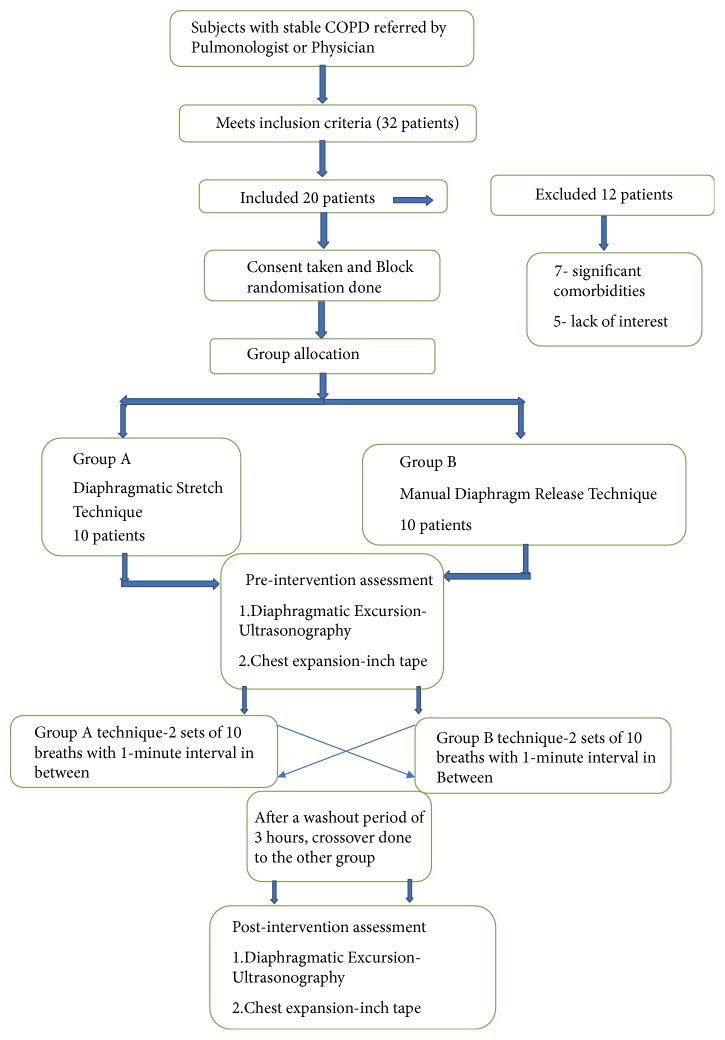
Materials and methods: This randomised crossover trial included 20 clinically stable patients with mild and moderate COPD classified according to the GOLD criteria. The patients were allocated to group A or group B by block randomization done by primary investigator. The information about the technique was concealed in a sealed opaque envelope and revealed to the patients only after allocation of groups. After taking the demographic data and baseline values of the outcome measures (diaphragm mobility by ultrasonography performed by an experienced radiologist and chest expansion by inch tape performed by the therapist), group A subjects underwent the diaphragmatic stretch technique and the group B subjects underwent the manual diaphragm release technique. Both the interventions were performed in 2 sets of 10 deep breaths with 1-minute interval between the sets. The two outcome variables were recorded immediately after the intervention. A wash-out period of 3 hours was maintained to neutralize the effect of given intervention. Later the patients of group A and group B were crossed over to the other group.
Results: In the diaphragmatic stretch technique, there was a statistically significant improvement in the diaphragmatic excursion before and after the treatment. On the right side, p=0.00 and p=0.003 in the midclavicular line and midaxillary line. On the left side, p=0.004 and p=0.312 in the midclavicular and midaxillary line. In manual diaphragm release technique, there was a statistically significant improvement before and after the treatment. On the right side, p=0.000 and p=0.000 in the midclavicular line and midaxillary line. On the left side, p=0.002 and p=0.000 in the midclavicular line and midaxillary line. There was no statistically significant difference in diaphragmatic excursion in the comparison of the postintervention values of both techniques.
Conclusion: The diaphragmatic stretch technique and manual diaphragm release technique can be safely recommended for patients with clinically stable COPD to improve diaphragmatic excursion.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


