Phase II study of ERC1671 plus bevacizumab versus bevacizumab plus placebo in recurrent glioblastoma: interim results and correlations with CD4+ T-lymphocyte counts.
Daniela A Bota, Jinah Chung, Manisha Dandekar, Jose A Carrillo, Xiao-Tang Kong, Beverly D Fu, Frank Pk Hsu, Axel H Schönthal, Florence M Hofman, Thomas C Chen, Raphael Zidovetzki, Chrystel Pretto, Ankie Strik, Virgil Ejc Schijns, Apostolos Stathopoulos
{"title":"Phase II study of ERC1671 plus bevacizumab versus bevacizumab plus placebo in recurrent glioblastoma: interim results and correlations with CD4<sup>+</sup> T-lymphocyte counts.","authors":"Daniela A Bota, Jinah Chung, Manisha Dandekar, Jose A Carrillo, Xiao-Tang Kong, Beverly D Fu, Frank Pk Hsu, Axel H Schönthal, Florence M Hofman, Thomas C Chen, Raphael Zidovetzki, Chrystel Pretto, Ankie Strik, Virgil Ejc Schijns, Apostolos Stathopoulos","doi":"10.2217/cns-2018-0009","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>ERC1671 is an allogeneic/autologous therapeutic glioblastoma (GBM) vaccine - composed of whole, inactivated tumor cells mixed with tumor cell lysates derived from the patient and three GBM donors.</p><p><strong>Methods: </strong>In this double-blinded, randomized, Phase II study bevacizumab-naive patients with recurrent GBM were randomized to receive either ERC1671 in combination with granulocyte-macrophage colony-stimulating factor (GM-CSF) (Leukine<sup>®</sup> or sargramostim) and cyclophosphamide plus bevacizumab, or placebo plus bevacizumab. Interim results: Median overall survival (OS) of patients treated with ERC1671 plus bevacizumab was 12 months. In the placebo plus bevacizumab group, median OS was 7.5 months. The maximal CD4<sup>+</sup> T-lymphocyte count correlated with OS in the ERC1671 but not in the placebo group.</p><p><strong>Conclusion: </strong>The addition of ERC1671/GM-CSF/cyclophosphamide to bevacizumab resulted in a clinically meaningful survival benefit with minimal additional toxicity.</p>","PeriodicalId":10469,"journal":{"name":"CNS Oncology","volume":"7 3","pages":"CNS22"},"PeriodicalIF":0.0000,"publicationDate":"2018-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2217/cns-2018-0009","citationCount":"42","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CNS Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2217/cns-2018-0009","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/8/29 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 42
Abstract
Aim: ERC1671 is an allogeneic/autologous therapeutic glioblastoma (GBM) vaccine - composed of whole, inactivated tumor cells mixed with tumor cell lysates derived from the patient and three GBM donors.
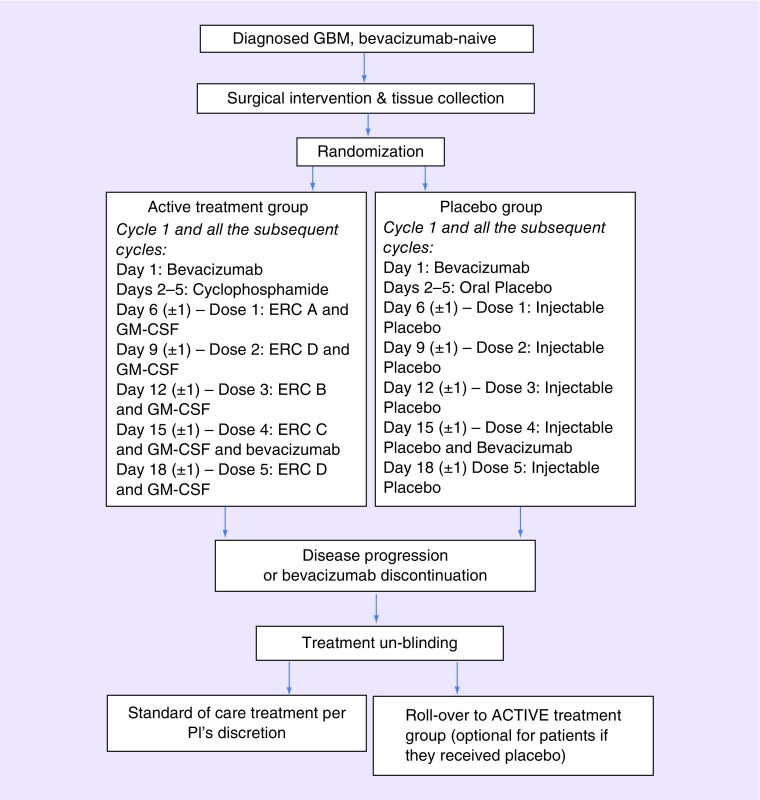
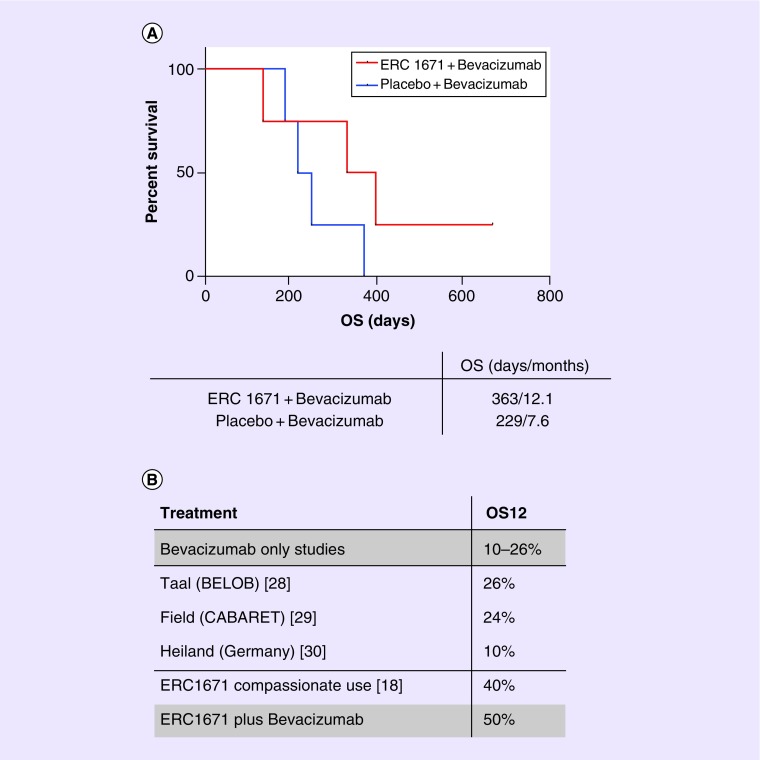
Methods: In this double-blinded, randomized, Phase II study bevacizumab-naive patients with recurrent GBM were randomized to receive either ERC1671 in combination with granulocyte-macrophage colony-stimulating factor (GM-CSF) (Leukine® or sargramostim) and cyclophosphamide plus bevacizumab, or placebo plus bevacizumab. Interim results: Median overall survival (OS) of patients treated with ERC1671 plus bevacizumab was 12 months. In the placebo plus bevacizumab group, median OS was 7.5 months. The maximal CD4+ T-lymphocyte count correlated with OS in the ERC1671 but not in the placebo group.
Conclusion: The addition of ERC1671/GM-CSF/cyclophosphamide to bevacizumab resulted in a clinically meaningful survival benefit with minimal additional toxicity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


