Noor Shafina Mohd Nor, Choong Yi Fong, Kartini Rahmat, Wan Mun Vanessa Lee, Azriyanti Anuar Zaini, Muhammad Yazid Jalaludin
{"title":"Ischaemic Haemorrhagic Stroke in a Child with New Onset Type 1 Diabetes Mellitus.","authors":"Noor Shafina Mohd Nor, Choong Yi Fong, Kartini Rahmat, Wan Mun Vanessa Lee, Azriyanti Anuar Zaini, Muhammad Yazid Jalaludin","doi":"10.17925/EE.2018.14.1.59","DOIUrl":null,"url":null,"abstract":"<p><p>Cerebral oedema is the most common neurological complication of diabetic ketoacidosis (DKA). However, ischaemic and haemorrhagic brain injury has been reported infrequently. A 10-year old girl who was previously well presented with severe DKA. She was tachycardic with poor peripheral perfusion but normotensive. However, two fast boluses totalling 40 ml/kg normal saline were given. She was transferred to another hospital where she was intubated due to drowsiness. Rehydration fluid (maintenance and 48-hour correction for 7.5% dehydration) was started followed by insulin infusion. She was extubated within 24 hours of admission. Her ketosis resolved soon after and subcutaneous insulin was started. However, about 48 hours after admission, her Glasgow Coma Scale score dropped to 11/15 (E4M5V2) with expressive aphasia and upper motor neuron signs. One dose of mannitol was given. Her symptoms improved gradually and at 26-month follow-up she had a near-complete recovery with only minimal left lower limb weakness. Serial magnetic resonance imaging brain scans showed vascular ischaemic injury at the frontal-parietal watershed regions with haemorrhagic transformation. This case reiterates the importance of monitoring the neurological status of patient's with DKA closely for possible neurological complications including an ischaemic and haemorrhagic stroke.</p>","PeriodicalId":38860,"journal":{"name":"European Endocrinology","volume":"14 1","pages":"59-61"},"PeriodicalIF":0.0000,"publicationDate":"2018-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.17925/EE.2018.14.1.59","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17925/EE.2018.14.1.59","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/4/18 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 2
Abstract
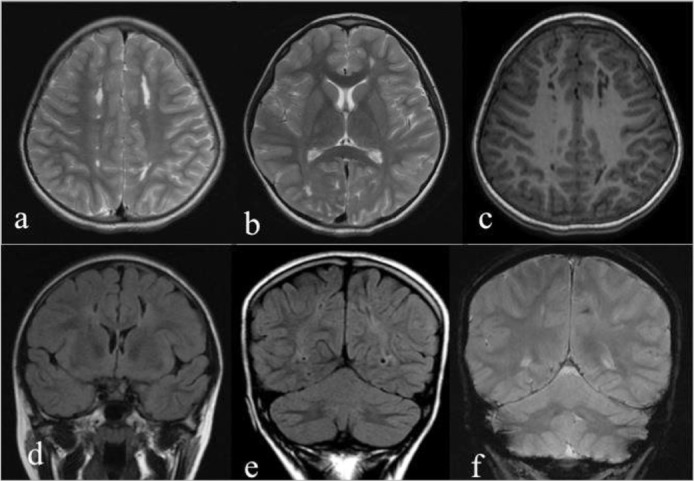
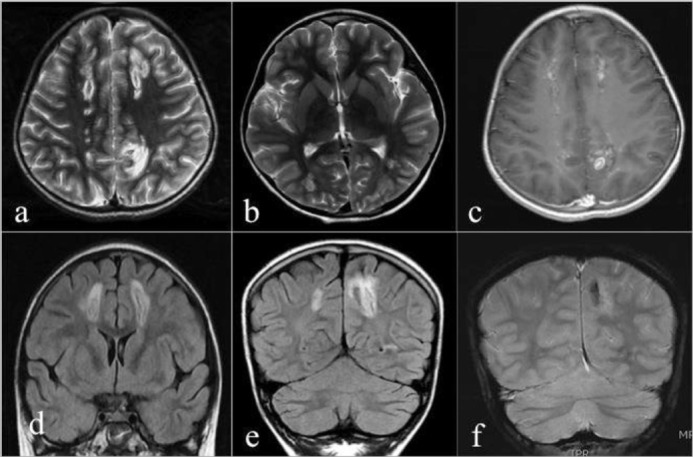
Cerebral oedema is the most common neurological complication of diabetic ketoacidosis (DKA). However, ischaemic and haemorrhagic brain injury has been reported infrequently. A 10-year old girl who was previously well presented with severe DKA. She was tachycardic with poor peripheral perfusion but normotensive. However, two fast boluses totalling 40 ml/kg normal saline were given. She was transferred to another hospital where she was intubated due to drowsiness. Rehydration fluid (maintenance and 48-hour correction for 7.5% dehydration) was started followed by insulin infusion. She was extubated within 24 hours of admission. Her ketosis resolved soon after and subcutaneous insulin was started. However, about 48 hours after admission, her Glasgow Coma Scale score dropped to 11/15 (E4M5V2) with expressive aphasia and upper motor neuron signs. One dose of mannitol was given. Her symptoms improved gradually and at 26-month follow-up she had a near-complete recovery with only minimal left lower limb weakness. Serial magnetic resonance imaging brain scans showed vascular ischaemic injury at the frontal-parietal watershed regions with haemorrhagic transformation. This case reiterates the importance of monitoring the neurological status of patient's with DKA closely for possible neurological complications including an ischaemic and haemorrhagic stroke.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


