K M Sharma, H Ranjani, A Zabetian, M Datta, M Deepa, C R Anand Moses, K M V Narayan, V Mohan, M K Ali
{"title":"Excess cost burden of diabetes in Southern India: a clinic-based, comparative cost-of-illness study.","authors":"K M Sharma, H Ranjani, A Zabetian, M Datta, M Deepa, C R Anand Moses, K M V Narayan, V Mohan, M K Ali","doi":"10.1017/gheg.2016.2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There are few data on excess direct and indirect costs of diabetes in India and limited data on rural costs of diabetes. We aimed to further explore these aspects of diabetes burdens using a clinic-based, comparative cost-of-illness study.</p><p><strong>Methods: </strong>Persons with diabetes (<i>n</i> = 606) were recruited from government, private, and rural clinics and compared to persons without diabetes matched for age, sex, and socioeconomic status (<i>n</i> = 356). We used interviewer-administered questionnaires to estimate direct costs (outpatient, inpatient, medication, laboratory, and procedures) and indirect costs [absence from (absenteeism) or low productivity at (presenteeism) work]. Excess costs were calculated as the difference between costs reported by persons with and without diabetes and compared across settings. Regression analyses were used to separately identify factors associated with total direct and indirect costs.</p><p><strong>Results: </strong>Annual excess direct costs were highest amongst private clinic attendees (INR 19 552, US$425) and lowest amongst government clinic attendees (INR 1204, US$26.17). Private clinic attendees had the lowest excess absenteeism (2.36 work days/year) and highest presenteeism (0.06 work days/year) due to diabetes. Government clinic attendees reported the highest absenteeism (7.48 work days/year) and lowest presenteeism (-0.31 work days/year). Ten additional years of diabetes duration was associated with 11% higher direct costs (<i>p</i> < 0.001). Older age (<i>p</i> = 0.02) and longer duration of diabetes (<i>p</i> < 0.001) were associated with higher total lost work days.</p><p><strong>Conclusions: </strong>Excess health expenditures and lost productivity amongst individuals with diabetes are substantial and different across care settings. Innovative solutions are needed to cope with diabetes and its associated cost burdens in India.</p>","PeriodicalId":44052,"journal":{"name":"Global Health Epidemiology and Genomics","volume":"1 ","pages":"e8"},"PeriodicalIF":1.1000,"publicationDate":"2016-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1017/gheg.2016.2","citationCount":"17","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Health Epidemiology and Genomics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1017/gheg.2016.2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 17
Abstract
Background: There are few data on excess direct and indirect costs of diabetes in India and limited data on rural costs of diabetes. We aimed to further explore these aspects of diabetes burdens using a clinic-based, comparative cost-of-illness study.
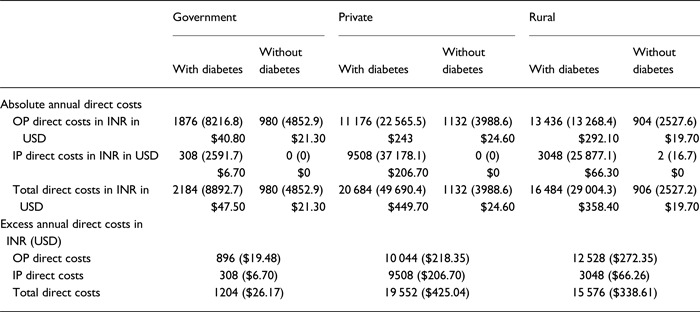
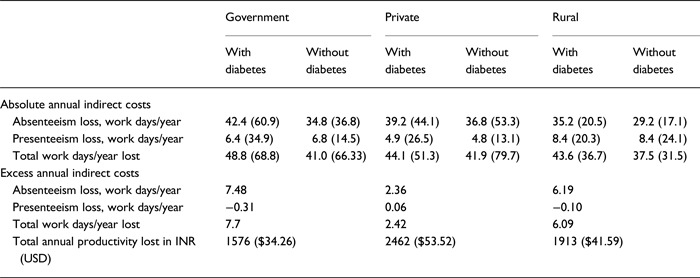
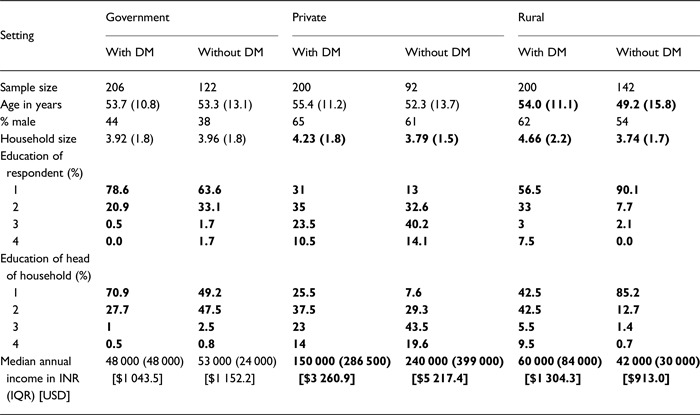
Methods: Persons with diabetes (n = 606) were recruited from government, private, and rural clinics and compared to persons without diabetes matched for age, sex, and socioeconomic status (n = 356). We used interviewer-administered questionnaires to estimate direct costs (outpatient, inpatient, medication, laboratory, and procedures) and indirect costs [absence from (absenteeism) or low productivity at (presenteeism) work]. Excess costs were calculated as the difference between costs reported by persons with and without diabetes and compared across settings. Regression analyses were used to separately identify factors associated with total direct and indirect costs.
Results: Annual excess direct costs were highest amongst private clinic attendees (INR 19 552, US$425) and lowest amongst government clinic attendees (INR 1204, US$26.17). Private clinic attendees had the lowest excess absenteeism (2.36 work days/year) and highest presenteeism (0.06 work days/year) due to diabetes. Government clinic attendees reported the highest absenteeism (7.48 work days/year) and lowest presenteeism (-0.31 work days/year). Ten additional years of diabetes duration was associated with 11% higher direct costs (p < 0.001). Older age (p = 0.02) and longer duration of diabetes (p < 0.001) were associated with higher total lost work days.
Conclusions: Excess health expenditures and lost productivity amongst individuals with diabetes are substantial and different across care settings. Innovative solutions are needed to cope with diabetes and its associated cost burdens in India.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


