B-chronic lymphocytic leukemia showed triple transformation, to diffuse large B cell, CD20-negative, and T-cell neoplasm during ofatumumab treatment: a case report.
{"title":"B-chronic lymphocytic leukemia showed triple transformation, to diffuse large B cell, CD20-negative, and T-cell neoplasm during ofatumumab treatment: a case report.","authors":"Osamu Imataki, Makiko Uemura","doi":"10.1186/s12907-018-0072-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic lymphocytic leukemia (CLL) is a mature lymphoid neoplasm currently categorized as an indolent type of malignant lymphoma. CLL progresses slowly over years, but it eventually transforms to a more aggressive lymphoma such as the diffuse large B-cell (DLBCL) type, also known as Richter's syndrome.</p><p><strong>Case presentation: </strong>We treated a 69-year-old Japanese male who was histologically diagnosed with Richter's syndrome after 6 years of CLL. His lymphadenopathy had systemically progressed for years, with lymphocyte counts of less than 10,000 cells/μL and a disease status of Rai classification stage I and Binet classification B. He had high fever and hepatosplenomegaly upon Richter's transformation. The patient was treated with ofatumumab for refractory CLL, which relieved his febrile lymphadenopathy. He received a total of 11 ofatumumab courses and achieved partial remission. On the day of the 12th course of ofatumumab, his disease relapsed with febrile lymphadenopathy. Computed tomography revealed multiple liver masses and systemic lymphadenopathy, while a liver biopsy confirmed T-cell lymphoma. Concomitantly, CD20-lacking CLL cells were detected in his peripheral blood and bone marrow, and pathological examination of his left cervical lymph node biopsy showed CD20-positive DLBCL. The final diagnosis was three different types of lymphoma pathologies: (1) CD20-positive DLBCL of the lymph nodes, (2) CD20-lacking CLL of the peripheral blood and bone marrow, and (3) peripheral T-cell lymphoma (PTCL) of the liver. He received intravenous and oral dexamethasone therapy as palliative care. He died because of the rapid progression of abdominal masses 2 months after the diagnosis of triple transformation CLL. An autopsy revealed aggressive PTCL with aggressive systemic involvement of the liver, spleen, gall bladder, pericardium, bone marrow, and mediastinal-paraaortic-intraceliac lymph nodes. T-cell receptor study of an autopsy specimen supported the diagnosis of PTCL that spread to the intraceliac organs and lymph nodes. We concluded that his pathogenicity progressed to a mixture of triple lymphoma as a result of double malignant transformations, which included PTCL from CLL, CD20-negative CLL, and CD20-positive DLBCL by Richter's transformation.</p><p><strong>Conclusions: </strong>Our case provides information on the biology of CLL, to transform from a low-grade chemosensitive status to a malignant chemoresistant status.</p>","PeriodicalId":35804,"journal":{"name":"BMC Clinical Pathology","volume":"18 ","pages":"5"},"PeriodicalIF":0.0000,"publicationDate":"2018-05-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s12907-018-0072-5","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Clinical Pathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12907-018-0072-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Chronic lymphocytic leukemia (CLL) is a mature lymphoid neoplasm currently categorized as an indolent type of malignant lymphoma. CLL progresses slowly over years, but it eventually transforms to a more aggressive lymphoma such as the diffuse large B-cell (DLBCL) type, also known as Richter's syndrome.
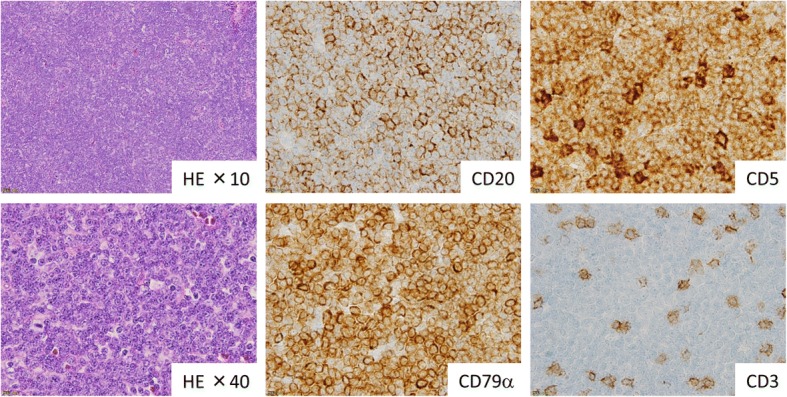
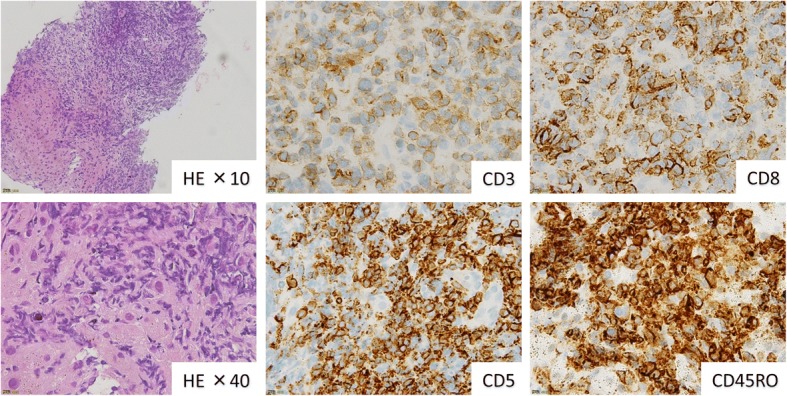
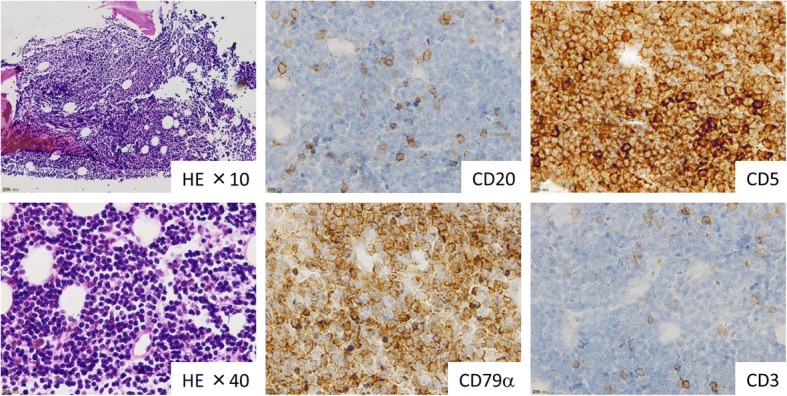
Case presentation: We treated a 69-year-old Japanese male who was histologically diagnosed with Richter's syndrome after 6 years of CLL. His lymphadenopathy had systemically progressed for years, with lymphocyte counts of less than 10,000 cells/μL and a disease status of Rai classification stage I and Binet classification B. He had high fever and hepatosplenomegaly upon Richter's transformation. The patient was treated with ofatumumab for refractory CLL, which relieved his febrile lymphadenopathy. He received a total of 11 ofatumumab courses and achieved partial remission. On the day of the 12th course of ofatumumab, his disease relapsed with febrile lymphadenopathy. Computed tomography revealed multiple liver masses and systemic lymphadenopathy, while a liver biopsy confirmed T-cell lymphoma. Concomitantly, CD20-lacking CLL cells were detected in his peripheral blood and bone marrow, and pathological examination of his left cervical lymph node biopsy showed CD20-positive DLBCL. The final diagnosis was three different types of lymphoma pathologies: (1) CD20-positive DLBCL of the lymph nodes, (2) CD20-lacking CLL of the peripheral blood and bone marrow, and (3) peripheral T-cell lymphoma (PTCL) of the liver. He received intravenous and oral dexamethasone therapy as palliative care. He died because of the rapid progression of abdominal masses 2 months after the diagnosis of triple transformation CLL. An autopsy revealed aggressive PTCL with aggressive systemic involvement of the liver, spleen, gall bladder, pericardium, bone marrow, and mediastinal-paraaortic-intraceliac lymph nodes. T-cell receptor study of an autopsy specimen supported the diagnosis of PTCL that spread to the intraceliac organs and lymph nodes. We concluded that his pathogenicity progressed to a mixture of triple lymphoma as a result of double malignant transformations, which included PTCL from CLL, CD20-negative CLL, and CD20-positive DLBCL by Richter's transformation.
Conclusions: Our case provides information on the biology of CLL, to transform from a low-grade chemosensitive status to a malignant chemoresistant status.
期刊介绍:
BMC Clinical Pathology is an open access journal publishing original peer-reviewed research articles in all aspects of histopathology, haematology, clinical biochemistry, and medical microbiology (including virology, parasitology, and infection control). BMC Clinical Pathology (ISSN 1472-6890) is indexed/tracked/covered by PubMed, CAS, EMBASE, Scopus and Google Scholar.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


