Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years - Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014.
IF 37.3 1区 医学Q1 PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH
Jon Baio, Lisa Wiggins, Deborah L Christensen, Matthew J Maenner, Julie Daniels, Zachary Warren, Margaret Kurzius-Spencer, Walter Zahorodny, Cordelia Robinson Rosenberg, Tiffany White, Maureen S Durkin, Pamela Imm, Loizos Nikolaou, Marshalyn Yeargin-Allsopp, Li-Ching Lee, Rebecca Harrington, Maya Lopez, Robert T Fitzgerald, Amy Hewitt, Sydney Pettygrove, John N Constantino, Alison Vehorn, Josephine Shenouda, Jennifer Hall-Lande, Kim Van Naarden Braun, Nicole F Dowling
{"title":"Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years - Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014.","authors":"Jon Baio, Lisa Wiggins, Deborah L Christensen, Matthew J Maenner, Julie Daniels, Zachary Warren, Margaret Kurzius-Spencer, Walter Zahorodny, Cordelia Robinson Rosenberg, Tiffany White, Maureen S Durkin, Pamela Imm, Loizos Nikolaou, Marshalyn Yeargin-Allsopp, Li-Ching Lee, Rebecca Harrington, Maya Lopez, Robert T Fitzgerald, Amy Hewitt, Sydney Pettygrove, John N Constantino, Alison Vehorn, Josephine Shenouda, Jennifer Hall-Lande, Kim Van Naarden Braun, Nicole F Dowling","doi":"10.15585/mmwr.ss6706a1","DOIUrl":null,"url":null,"abstract":"<p><strong>Problem/condition: </strong>Autism spectrum disorder (ASD).</p><p><strong>Period covered: </strong>2014.</p><p><strong>Description of system: </strong>The Autism and Developmental Disabilities Monitoring (ADDM) Network is an active surveillance system that provides estimates of the prevalence of autism spectrum disorder (ASD) among children aged 8 years whose parents or guardians reside within 11 ADDM sites in the United States (Arizona, Arkansas, Colorado, Georgia, Maryland, Minnesota, Missouri, New Jersey, North Carolina, Tennessee, and Wisconsin). ADDM surveillance is conducted in two phases. The first phase involves review and abstraction of comprehensive evaluations that were completed by professional service providers in the community. Staff completing record review and abstraction receive extensive training and supervision and are evaluated according to strict reliability standards to certify effective initial training, identify ongoing training needs, and ensure adherence to the prescribed methodology. Record review and abstraction occurs in a variety of data sources ranging from general pediatric health clinics to specialized programs serving children with developmental disabilities. In addition, most of the ADDM sites also review records for children who have received special education services in public schools. In the second phase of the study, all abstracted information is reviewed systematically by experienced clinicians to determine ASD case status. A child is considered to meet the surveillance case definition for ASD if he or she displays behaviors, as described on one or more comprehensive evaluations completed by community-based professional providers, consistent with the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) diagnostic criteria for autistic disorder; pervasive developmental disorder-not otherwise specified (PDD-NOS, including atypical autism); or Asperger disorder. This report provides updated ASD prevalence estimates for children aged 8 years during the 2014 surveillance year, on the basis of DSM-IV-TR criteria, and describes characteristics of the population of children with ASD. In 2013, the American Psychiatric Association published the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), which made considerable changes to ASD diagnostic criteria. The change in ASD diagnostic criteria might influence ADDM ASD prevalence estimates; therefore, most (85%) of the records used to determine prevalence estimates based on DSM-IV-TR criteria underwent additional review under a newly operationalized surveillance case definition for ASD consistent with the DSM-5 diagnostic criteria. Children meeting this new surveillance case definition could qualify on the basis of one or both of the following criteria, as documented in abstracted comprehensive evaluations: 1) behaviors consistent with the DSM-5 diagnostic features; and/or 2) an ASD diagnosis, whether based on DSM-IV-TR or DSM-5 diagnostic criteria. Stratified comparisons of the number of children meeting either of these two case definitions also are reported.</p><p><strong>Results: </strong>For 2014, the overall prevalence of ASD among the 11 ADDM sites was 16.8 per 1,000 (one in 59) children aged 8 years. Overall ASD prevalence estimates varied among sites, from 13.1-29.3 per 1,000 children aged 8 years. ASD prevalence estimates also varied by sex and race/ethnicity. Males were four times more likely than females to be identified with ASD. Prevalence estimates were higher for non-Hispanic white (henceforth, white) children compared with non-Hispanic black (henceforth, black) children, and both groups were more likely to be identified with ASD compared with Hispanic children. Among the nine sites with sufficient data on intellectual ability, 31% of children with ASD were classified in the range of intellectual disability (intelligence quotient [IQ] <70), 25% were in the borderline range (IQ 71-85), and 44% had IQ scores in the average to above average range (i.e., IQ >85). The distribution of intellectual ability varied by sex and race/ethnicity. Although mention of developmental concerns by age 36 months was documented for 85% of children with ASD, only 42% had a comprehensive evaluation on record by age 36 months. The median age of earliest known ASD diagnosis was 52 months and did not differ significantly by sex or race/ethnicity. For the targeted comparison of DSM-IV-TR and DSM-5 results, the number and characteristics of children meeting the newly operationalized DSM-5 case definition for ASD were similar to those meeting the DSM-IV-TR case definition, with DSM-IV-TR case counts exceeding DSM-5 counts by less than 5% and approximately 86% overlap between the two case definitions (kappa = 0.85).</p><p><strong>Interpretation: </strong>Findings from the ADDM Network, on the basis of 2014 data reported from 11 sites, provide updated population-based estimates of the prevalence of ASD among children aged 8 years in multiple communities in the United States. The overall ASD prevalence estimate of 16.8 per 1,000 children aged 8 years in 2014 is higher than previously reported estimates from the ADDM Network. Because the ADDM sites do not provide a representative sample of the entire United States, the combined prevalence estimates presented in this report cannot be generalized to all children aged 8 years in the United States. Consistent with reports from previous ADDM surveillance years, findings from 2014 were marked by variation in ASD prevalence when stratified by geographic area, sex, and level of intellectual ability. Differences in prevalence estimates between black and white children have diminished in most sites, but remained notable for Hispanic children. For 2014, results from application of the DSM-IV-TR and DSM-5 case definitions were similar, overall and when stratified by sex, race/ethnicity, DSM-IV-TR diagnostic subtype, or level of intellectual ability.</p><p><strong>Public health action: </strong>Beginning with surveillance year 2016, the DSM-5 case definition will serve as the basis for ADDM estimates of ASD prevalence in future surveillance reports. Although the DSM-IV-TR case definition will eventually be phased out, it will be applied in a limited geographic area to offer additional data for comparison. Future analyses will examine trends in the continued use of DSM-IV-TR diagnoses, such as autistic disorder, PDD-NOS, and Asperger disorder in health and education records, documentation of symptoms consistent with DSM-5 terminology, and how these trends might influence estimates of ASD prevalence over time. The latest findings from the ADDM Network provide evidence that the prevalence of ASD is higher than previously reported estimates and continues to vary among certain racial/ethnic groups and communities. With prevalence of ASD ranging from 13.1 to 29.3 per 1,000 children aged 8 years in different communities throughout the United States, the need for behavioral, educational, residential, and occupational services remains high, as does the need for increased research on both genetic and nongenetic risk factors for ASD.</p>","PeriodicalId":48549,"journal":{"name":"Mmwr Surveillance Summaries","volume":"67 6","pages":"1-23"},"PeriodicalIF":37.3000,"publicationDate":"2018-04-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.15585/mmwr.ss6706a1","citationCount":"3288","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mmwr Surveillance Summaries","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.15585/mmwr.ss6706a1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Description of system: The Autism and Developmental Disabilities Monitoring (ADDM) Network is an active surveillance system that provides estimates of the prevalence of autism spectrum disorder (ASD) among children aged 8 years whose parents or guardians reside within 11 ADDM sites in the United States (Arizona, Arkansas, Colorado, Georgia, Maryland, Minnesota, Missouri, New Jersey, North Carolina, Tennessee, and Wisconsin). ADDM surveillance is conducted in two phases. The first phase involves review and abstraction of comprehensive evaluations that were completed by professional service providers in the community. Staff completing record review and abstraction receive extensive training and supervision and are evaluated according to strict reliability standards to certify effective initial training, identify ongoing training needs, and ensure adherence to the prescribed methodology. Record review and abstraction occurs in a variety of data sources ranging from general pediatric health clinics to specialized programs serving children with developmental disabilities. In addition, most of the ADDM sites also review records for children who have received special education services in public schools. In the second phase of the study, all abstracted information is reviewed systematically by experienced clinicians to determine ASD case status. A child is considered to meet the surveillance case definition for ASD if he or she displays behaviors, as described on one or more comprehensive evaluations completed by community-based professional providers, consistent with the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) diagnostic criteria for autistic disorder; pervasive developmental disorder-not otherwise specified (PDD-NOS, including atypical autism); or Asperger disorder. This report provides updated ASD prevalence estimates for children aged 8 years during the 2014 surveillance year, on the basis of DSM-IV-TR criteria, and describes characteristics of the population of children with ASD. In 2013, the American Psychiatric Association published the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), which made considerable changes to ASD diagnostic criteria. The change in ASD diagnostic criteria might influence ADDM ASD prevalence estimates; therefore, most (85%) of the records used to determine prevalence estimates based on DSM-IV-TR criteria underwent additional review under a newly operationalized surveillance case definition for ASD consistent with the DSM-5 diagnostic criteria. Children meeting this new surveillance case definition could qualify on the basis of one or both of the following criteria, as documented in abstracted comprehensive evaluations: 1) behaviors consistent with the DSM-5 diagnostic features; and/or 2) an ASD diagnosis, whether based on DSM-IV-TR or DSM-5 diagnostic criteria. Stratified comparisons of the number of children meeting either of these two case definitions also are reported.
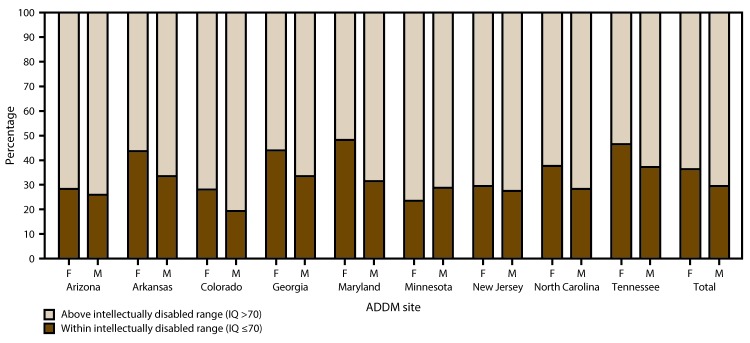
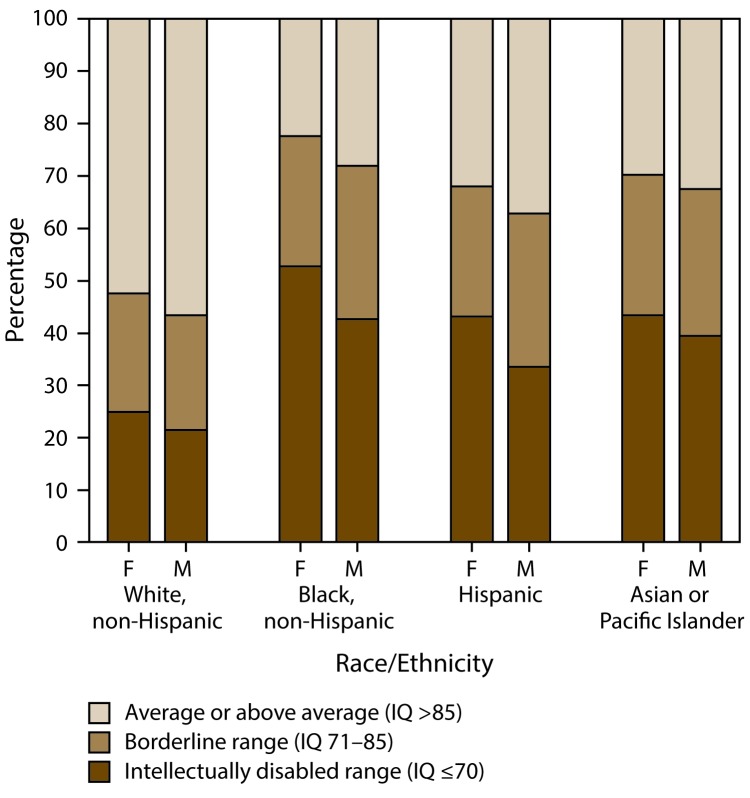
Results: For 2014, the overall prevalence of ASD among the 11 ADDM sites was 16.8 per 1,000 (one in 59) children aged 8 years. Overall ASD prevalence estimates varied among sites, from 13.1-29.3 per 1,000 children aged 8 years. ASD prevalence estimates also varied by sex and race/ethnicity. Males were four times more likely than females to be identified with ASD. Prevalence estimates were higher for non-Hispanic white (henceforth, white) children compared with non-Hispanic black (henceforth, black) children, and both groups were more likely to be identified with ASD compared with Hispanic children. Among the nine sites with sufficient data on intellectual ability, 31% of children with ASD were classified in the range of intellectual disability (intelligence quotient [IQ] <70), 25% were in the borderline range (IQ 71-85), and 44% had IQ scores in the average to above average range (i.e., IQ >85). The distribution of intellectual ability varied by sex and race/ethnicity. Although mention of developmental concerns by age 36 months was documented for 85% of children with ASD, only 42% had a comprehensive evaluation on record by age 36 months. The median age of earliest known ASD diagnosis was 52 months and did not differ significantly by sex or race/ethnicity. For the targeted comparison of DSM-IV-TR and DSM-5 results, the number and characteristics of children meeting the newly operationalized DSM-5 case definition for ASD were similar to those meeting the DSM-IV-TR case definition, with DSM-IV-TR case counts exceeding DSM-5 counts by less than 5% and approximately 86% overlap between the two case definitions (kappa = 0.85).
Interpretation: Findings from the ADDM Network, on the basis of 2014 data reported from 11 sites, provide updated population-based estimates of the prevalence of ASD among children aged 8 years in multiple communities in the United States. The overall ASD prevalence estimate of 16.8 per 1,000 children aged 8 years in 2014 is higher than previously reported estimates from the ADDM Network. Because the ADDM sites do not provide a representative sample of the entire United States, the combined prevalence estimates presented in this report cannot be generalized to all children aged 8 years in the United States. Consistent with reports from previous ADDM surveillance years, findings from 2014 were marked by variation in ASD prevalence when stratified by geographic area, sex, and level of intellectual ability. Differences in prevalence estimates between black and white children have diminished in most sites, but remained notable for Hispanic children. For 2014, results from application of the DSM-IV-TR and DSM-5 case definitions were similar, overall and when stratified by sex, race/ethnicity, DSM-IV-TR diagnostic subtype, or level of intellectual ability.
Public health action: Beginning with surveillance year 2016, the DSM-5 case definition will serve as the basis for ADDM estimates of ASD prevalence in future surveillance reports. Although the DSM-IV-TR case definition will eventually be phased out, it will be applied in a limited geographic area to offer additional data for comparison. Future analyses will examine trends in the continued use of DSM-IV-TR diagnoses, such as autistic disorder, PDD-NOS, and Asperger disorder in health and education records, documentation of symptoms consistent with DSM-5 terminology, and how these trends might influence estimates of ASD prevalence over time. The latest findings from the ADDM Network provide evidence that the prevalence of ASD is higher than previously reported estimates and continues to vary among certain racial/ethnic groups and communities. With prevalence of ASD ranging from 13.1 to 29.3 per 1,000 children aged 8 years in different communities throughout the United States, the need for behavioral, educational, residential, and occupational services remains high, as does the need for increased research on both genetic and nongenetic risk factors for ASD.
期刊介绍:
The Morbidity and Mortality Weekly Report (MMWR) Series, produced by the Centers for Disease Control and Prevention (CDC), is commonly referred to as "the voice of CDC." Serving as the primary outlet for timely, reliable, authoritative, accurate, objective, and practical public health information and recommendations, the MMWR is a crucial publication. Its readership primarily includes physicians, nurses, public health practitioners, epidemiologists, scientists, researchers, educators, and laboratorians.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


