{"title":"Intravenous lidocaine as adjuvant to general anesthesia in renal surgery.","authors":"Mohamed Said Nakhli, Mohamed Kahloul, Taieb Guizani, Chekib Zedini, Ajmi Chaouch, Walid Naija","doi":"10.1080/19932820.2018.1433418","DOIUrl":null,"url":null,"abstract":"<p><p>The role of intraoperative intravenous lidocaine infusion has been previously evaluated for pain relief, inflammatory response, and post-operative recovery, particularly in abdominal surgery. The present study is a randomized double-blinded trial in which we evaluated whether IV lidocaine infusion reduces isoflurane requirement, intraoperative remifentanil consumption and time to post-operative recovery in non-laparoscopic renal surgery. Sixty patients scheduled to undergo elective non-laparoscopic renal surgery under general anesthesia were enrolled to receive either systemic lidocaine infusion (group L: bolus 1.5 mg/kg followed by a continuous infusion at the rate of 2 mg/kg/hr until skin closure) or normal saline (0.9% NaCl solution) (Group C). The depth of anesthesia was monitored using the Bispectral Index Scale (BIS), which is based on measurement of the patient's cerebral electrical activity. Primary outcome of the study was End-tidal of isoflurane concentration (Et-Iso) at BIS values of 40-60. Secondary outcomes include remifentanil consumption during the operation and time to extubation. Et-Iso was significantly lower in group L than in group C (0.63% ± 0.10% vs 0.92% ± 0.11%, p < 10<sup>-3)</sup>. Mean remifentanil consumption of was significantly lower in group L than in group C (0.13 ± 0.04 µg/kg/min vs 0.18 ± 0.04 µg/kg/min, p < 10<sup>-3</sup>). Thus, IV lidocaine infusion permits a reduction of 31% in isoflurane concentration requirement and 27% in the intraoperative remifentanil need. In addition, recovery from anesthesia and extubation time was shorter in group L (5.8 ± 1.8 min vs 7.9 ± 2.0 min, p < 10<sup>-3</sup>). By reducing significantly isoflurane and remifentanil requirements during renal surgery, intravenous lidocaine could provide effective strategy to limit volatile agent and intraoperative opioids consumption especially in low and middle income countries.</p>","PeriodicalId":256060,"journal":{"name":"The Libyan Journal of Medicine","volume":" ","pages":"1433418"},"PeriodicalIF":0.0000,"publicationDate":"2018-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1080/19932820.2018.1433418","citationCount":"19","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Libyan Journal of Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/19932820.2018.1433418","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 19
Abstract
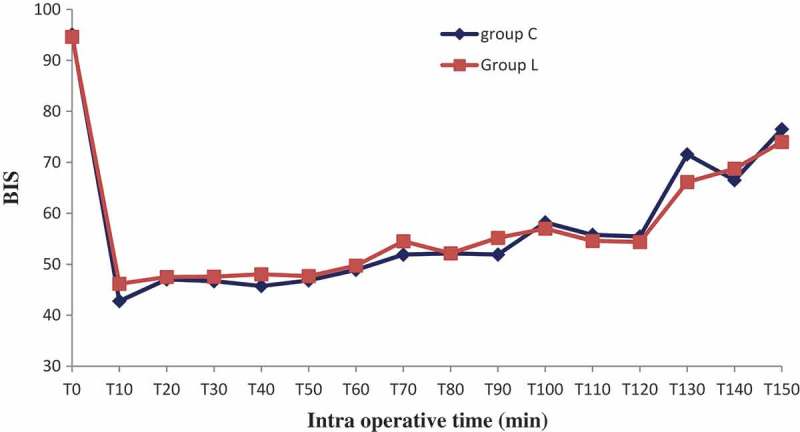
The role of intraoperative intravenous lidocaine infusion has been previously evaluated for pain relief, inflammatory response, and post-operative recovery, particularly in abdominal surgery. The present study is a randomized double-blinded trial in which we evaluated whether IV lidocaine infusion reduces isoflurane requirement, intraoperative remifentanil consumption and time to post-operative recovery in non-laparoscopic renal surgery. Sixty patients scheduled to undergo elective non-laparoscopic renal surgery under general anesthesia were enrolled to receive either systemic lidocaine infusion (group L: bolus 1.5 mg/kg followed by a continuous infusion at the rate of 2 mg/kg/hr until skin closure) or normal saline (0.9% NaCl solution) (Group C). The depth of anesthesia was monitored using the Bispectral Index Scale (BIS), which is based on measurement of the patient's cerebral electrical activity. Primary outcome of the study was End-tidal of isoflurane concentration (Et-Iso) at BIS values of 40-60. Secondary outcomes include remifentanil consumption during the operation and time to extubation. Et-Iso was significantly lower in group L than in group C (0.63% ± 0.10% vs 0.92% ± 0.11%, p < 10-3). Mean remifentanil consumption of was significantly lower in group L than in group C (0.13 ± 0.04 µg/kg/min vs 0.18 ± 0.04 µg/kg/min, p < 10-3). Thus, IV lidocaine infusion permits a reduction of 31% in isoflurane concentration requirement and 27% in the intraoperative remifentanil need. In addition, recovery from anesthesia and extubation time was shorter in group L (5.8 ± 1.8 min vs 7.9 ± 2.0 min, p < 10-3). By reducing significantly isoflurane and remifentanil requirements during renal surgery, intravenous lidocaine could provide effective strategy to limit volatile agent and intraoperative opioids consumption especially in low and middle income countries.
术中静脉输注利多卡因在缓解疼痛、炎症反应和术后恢复方面的作用已被评估,特别是在腹部手术中。本研究是一项随机双盲试验,我们评估了静脉输注利多卡因是否减少了非腹腔镜肾手术中异氟醚的需求、术中瑞芬太尼的消耗和术后恢复时间。60例计划在全麻下进行选择性非腹腔镜肾手术的患者,接受全身利多卡因输注(L组:静脉注射1.5 mg/kg,然后以2 mg/kg/hr的速度持续输注,直到皮肤闭合)或生理盐水(0.9% NaCl溶液)(C组)。麻醉深度采用双谱指数量表(BIS)监测,该量表基于患者脑电活动的测量。本研究的主要终点是BIS值为40-60时异氟烷浓度(Et-Iso)的末潮值。次要结果包括手术期间瑞芬太尼的消耗和拔管时间。L组Et-Iso显著低于C组(0.63%±0.10% vs 0.92%±0.11%,p -3)。L组的瑞芬太尼平均消耗量显著低于C组(0.13±0.04µg/kg/min vs 0.18±0.04µg/kg/min, p -3)。因此,静脉输注利多卡因可使异氟烷浓度需求降低31%,术中瑞芬太尼需求降低27%。此外,L组麻醉恢复和拔管时间较短(5.8±1.8 min vs 7.9±2.0 min, p -3)。通过在肾脏手术期间显著减少异氟醚和瑞芬太尼的需求,静脉注射利多卡因可以提供有效的策略来限制挥发性剂和术中阿片类药物的消耗,特别是在低收入和中等收入国家。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


