BRCA Genetic Testing and Receipt of Preventive Interventions Among Women Aged 18-64 Years with Employer-Sponsored Health Insurance in Nonmetropolitan and Metropolitan Areas - United States, 2009-2014.
IF 37.3 1区 医学Q1 PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH
Katherine Kolor, Zhuo Chen, Scott D Grosse, Juan L Rodriguez, Ridgely Fisk Green, W David Dotson, M Scott Bowen, Julie A Lynch, Muin J Khoury
{"title":"BRCA Genetic Testing and Receipt of Preventive Interventions Among Women Aged 18-64 Years with Employer-Sponsored Health Insurance in Nonmetropolitan and Metropolitan Areas - United States, 2009-2014.","authors":"Katherine Kolor, Zhuo Chen, Scott D Grosse, Juan L Rodriguez, Ridgely Fisk Green, W David Dotson, M Scott Bowen, Julie A Lynch, Muin J Khoury","doi":"10.15585/mmwr.ss6615a1","DOIUrl":null,"url":null,"abstract":"<p><strong>Problem/condition: </strong>Genetic testing for breast cancer 1 (BRCA1) and breast cancer 2 (BRCA2) gene mutations can identify women at increased risk for breast and ovarian cancer. These testing results can be used to select preventive interventions and guide treatment. Differences between nonmetropolitan and metropolitan populations in rates of BRCA testing and receipt of preventive interventions after testing have not previously been examined.</p><p><strong>Period covered: </strong>2009-2014.</p><p><strong>Description of system: </strong>Medical claims data from Truven Health Analytics MarketScan Commercial Claims and Encounters databases were used to estimate rates of BRCA testing and receipt of preventive interventions after BRCA testing among women aged 18-64 years with employer-sponsored health insurance in metropolitan and nonmetropolitan areas of the United States, both nationally and regionally.</p><p><strong>Results: </strong>From 2009 to 2014, BRCA testing rates per 100,000 women aged 18-64 years with employer-sponsored health insurance increased 2.3 times (102.7 to 237.8) in metropolitan areas and 3.0 times (64.8 to 191.3) in nonmetropolitan areas. The relative difference in BRCA testing rates between metropolitan and nonmetropolitan areas decreased from 37% in 2009 (102.7 versus 64.8) to 20% in 2014 (237.8 versus 191.3). The relative difference in BRCA testing rates between metropolitan and nonmetropolitan areas decreased more over time in younger women than in older women and decreased in all regions except the West. Receipt of preventive services 90 days after BRCA testing in metropolitan versus nonmetropolitan areas throughout the period varied by service: the percentage of women who received a mastectomy was similar, the percentage of women who received magnetic resonance imaging of the breast was lower in nonmetropolitan areas (as low as 5.8% in 2014 to as high as 8.2% in 2011) than metropolitan areas (as low as 7.3% in 2014 to as high as 10.3% in 2011), and the percentage of women who received mammography was lower in nonmetropolitan areas in earlier years but was similar in later years.</p><p><strong>Interpretation: </strong>Possible explanations for the 47% decrease in the relative difference in BRCA testing rates over the study period include increased access to genetic services in nonmetropolitan areas and increased demand nationally as a result of publicity. The relative differences in metropolitan and nonmetropolitan BRCA testing rates were smaller among women at younger ages compared with older ages.</p><p><strong>Public health action: </strong>Improved data sources and surveillance tools are needed to gather comprehensive data on BRCA testing in the United States, monitor adherence to evidence-based guidelines for BRCA testing, and assess receipt of preventive interventions for women with BRCA mutations. Programs can build on the recent decrease in geographic disparities in receipt of BRCA testing while simultaneously educating the public and health care providers about U.S. Preventive Services Task Force recommendations and other clinical guidelines for BRCA testing and counseling.</p>","PeriodicalId":48549,"journal":{"name":"Mmwr Surveillance Summaries","volume":"66 15","pages":"1-11"},"PeriodicalIF":37.3000,"publicationDate":"2017-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5879728/pdf/","citationCount":"59","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mmwr Surveillance Summaries","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.15585/mmwr.ss6615a1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 59
Abstract
Problem/condition: Genetic testing for breast cancer 1 (BRCA1) and breast cancer 2 (BRCA2) gene mutations can identify women at increased risk for breast and ovarian cancer. These testing results can be used to select preventive interventions and guide treatment. Differences between nonmetropolitan and metropolitan populations in rates of BRCA testing and receipt of preventive interventions after testing have not previously been examined.
Period covered: 2009-2014.
Description of system: Medical claims data from Truven Health Analytics MarketScan Commercial Claims and Encounters databases were used to estimate rates of BRCA testing and receipt of preventive interventions after BRCA testing among women aged 18-64 years with employer-sponsored health insurance in metropolitan and nonmetropolitan areas of the United States, both nationally and regionally.
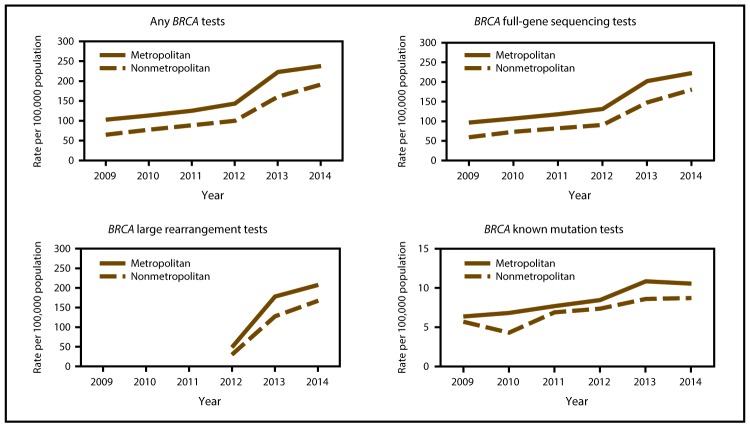
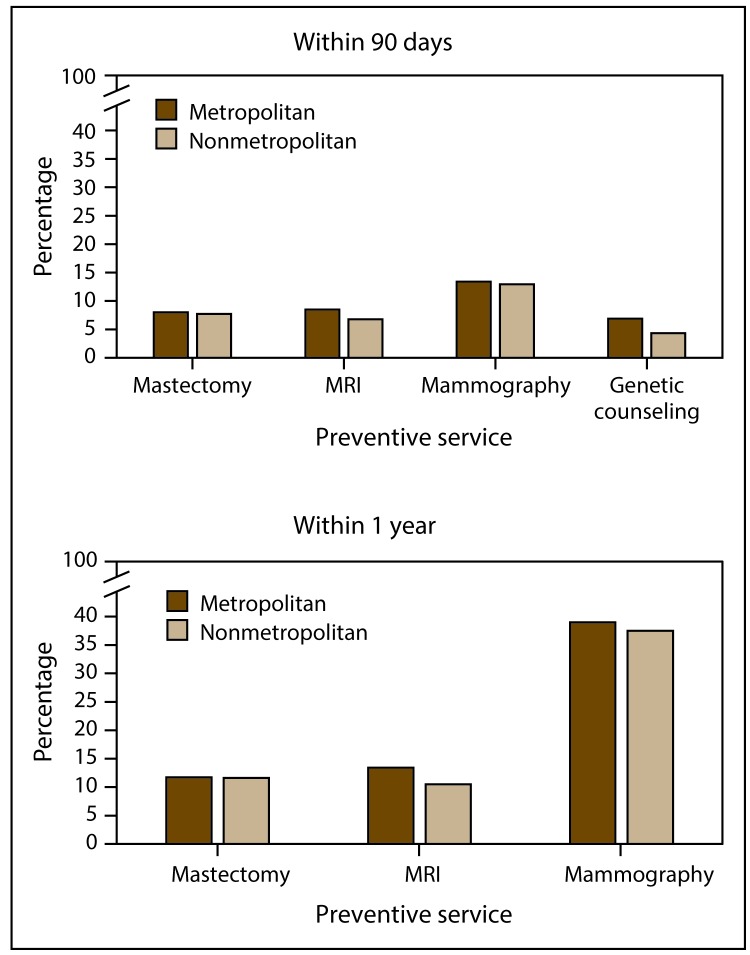
Results: From 2009 to 2014, BRCA testing rates per 100,000 women aged 18-64 years with employer-sponsored health insurance increased 2.3 times (102.7 to 237.8) in metropolitan areas and 3.0 times (64.8 to 191.3) in nonmetropolitan areas. The relative difference in BRCA testing rates between metropolitan and nonmetropolitan areas decreased from 37% in 2009 (102.7 versus 64.8) to 20% in 2014 (237.8 versus 191.3). The relative difference in BRCA testing rates between metropolitan and nonmetropolitan areas decreased more over time in younger women than in older women and decreased in all regions except the West. Receipt of preventive services 90 days after BRCA testing in metropolitan versus nonmetropolitan areas throughout the period varied by service: the percentage of women who received a mastectomy was similar, the percentage of women who received magnetic resonance imaging of the breast was lower in nonmetropolitan areas (as low as 5.8% in 2014 to as high as 8.2% in 2011) than metropolitan areas (as low as 7.3% in 2014 to as high as 10.3% in 2011), and the percentage of women who received mammography was lower in nonmetropolitan areas in earlier years but was similar in later years.
Interpretation: Possible explanations for the 47% decrease in the relative difference in BRCA testing rates over the study period include increased access to genetic services in nonmetropolitan areas and increased demand nationally as a result of publicity. The relative differences in metropolitan and nonmetropolitan BRCA testing rates were smaller among women at younger ages compared with older ages.
Public health action: Improved data sources and surveillance tools are needed to gather comprehensive data on BRCA testing in the United States, monitor adherence to evidence-based guidelines for BRCA testing, and assess receipt of preventive interventions for women with BRCA mutations. Programs can build on the recent decrease in geographic disparities in receipt of BRCA testing while simultaneously educating the public and health care providers about U.S. Preventive Services Task Force recommendations and other clinical guidelines for BRCA testing and counseling.
期刊介绍:
The Morbidity and Mortality Weekly Report (MMWR) Series, produced by the Centers for Disease Control and Prevention (CDC), is commonly referred to as "the voice of CDC." Serving as the primary outlet for timely, reliable, authoritative, accurate, objective, and practical public health information and recommendations, the MMWR is a crucial publication. Its readership primarily includes physicians, nurses, public health practitioners, epidemiologists, scientists, researchers, educators, and laboratorians.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


