Sero-diagnosis of Active Mycobacterium tuberculosis Disease among HIV Co-infected Persons using Thymidylate Kinase based Antigen and Antibody Capture Enzyme Immuno-Assays.
Misaki Wayengera, Ivan Mwebaza, Johnson Welishe, Cynthia Nakimuli, David P Kateete, Eddie Wampande, Samuel Kirimunda, Lois Bayigga, Carol Musubika, Peace Babirye, Benon Asiimwe, Moses L Joloba
{"title":"Sero-diagnosis of Active <i>Mycobacterium tuberculosis</i> Disease among HIV Co-infected Persons using Thymidylate Kinase based Antigen and Antibody Capture Enzyme Immuno-Assays.","authors":"Misaki Wayengera, Ivan Mwebaza, Johnson Welishe, Cynthia Nakimuli, David P Kateete, Eddie Wampande, Samuel Kirimunda, Lois Bayigga, Carol Musubika, Peace Babirye, Benon Asiimwe, Moses L Joloba","doi":"10.4172/2161-1068.1000241","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Clinical and laboratory diagnosis of Active Tuberculosis (ATB) and latent <i>Mycobacterium Tuberculosis</i> (<i>M. tuberculosis</i>) infections (LTBI) among people living with HIV/AIDS (PLWHA) presents formidable challenges. In the past, WHO issued an advisory against the use of existing TB sero-diagnostics. Emerging evidence, however, points to a precision of TB sero-diagnostics based on secretory rather than structural <i>M. tuberculosis</i> antigens. We hypothesized that secretory levels of <i>M. tuberculosis</i> thymidylate kinase (TMKmt) can Designate ATBI from LTBI and no TB (NTB). Here, we report in-house validation studies of levels of TMKmt antigen (Ag) and host specific TMKmt antibody (Ab) amongst HIV +ve and HIV -ve participants.</p><p><strong>Methods and results: </strong>Direct TMKmt Ag and host specific IgG Ab detection EIAs were conducted on broadly consented, stored serum (N=281[Ag] <i>vs</i>. 214 [Ab] respective) samples stratified as either HIV +ve or HIV-ve ATB relative to LTBI and No TB. On one hand, UG-peptide 1 and its PAb-based EIAs accurately diagnosed ATB relative to LTBI and NTB among HIV +ve subjects {irrespectively: (a) Ag detection ATB=OD>0.490; 95% CI: 0.7446 to 0.8715 <i>vs</i>. LTBI=OD<0.490; 95% CI 0.4325 to 0.4829 <i>vs</i>. NTB=OD<0.26; 95% CI 0.1675 to 0.2567 and (b) TMKmt specific IgG detection ATB=OD>1.00; 95% CI 1.170 to 1.528 [HIV +ve] and 2.044 to 2.978 [HIV -ve] respectively <i>vs</i>. LTBI=OD<1.00; 95% CI 0.2690 to 0.6396 <i>vs</i>. NTB=OD<; 95% CI 0.1527 to 0.8751}. HIV -ve ATB presented with Ag levels greater than NTB and less than LTBI (i.e. ATB -ve=<0.490 ODs>0.26), but displayed better ant-TMKmt IgG responses (OD>2.00; 95% CI 2.044 to 2.978) relative to HIV +ve ATB (OD<1.600; 95% CI 1.170 to 1.528); suggesting a better control of <i>M. tuberculosis</i>-septicemia. On the other hand, UG-peptide 2 and its PAb-based EIAs did not demonstrate ATB diagnostic potential regardless of HIV sero-status, except towards designating NTB.</p><p><strong>Conclusions: </strong>TMKmt Ab and Ag detecting EIAs based on UG-peptide 1 and its derivative PAb can accurately demarcate ATB from LTBI and NTB among HIV +ve subjects.</p>","PeriodicalId":74235,"journal":{"name":"Mycobacterial diseases : tuberculosis & leprosy","volume":"7 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2017-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5573238/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mycobacterial diseases : tuberculosis & leprosy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4172/2161-1068.1000241","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/5/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Clinical and laboratory diagnosis of Active Tuberculosis (ATB) and latent Mycobacterium Tuberculosis (M. tuberculosis) infections (LTBI) among people living with HIV/AIDS (PLWHA) presents formidable challenges. In the past, WHO issued an advisory against the use of existing TB sero-diagnostics. Emerging evidence, however, points to a precision of TB sero-diagnostics based on secretory rather than structural M. tuberculosis antigens. We hypothesized that secretory levels of M. tuberculosis thymidylate kinase (TMKmt) can Designate ATBI from LTBI and no TB (NTB). Here, we report in-house validation studies of levels of TMKmt antigen (Ag) and host specific TMKmt antibody (Ab) amongst HIV +ve and HIV -ve participants.
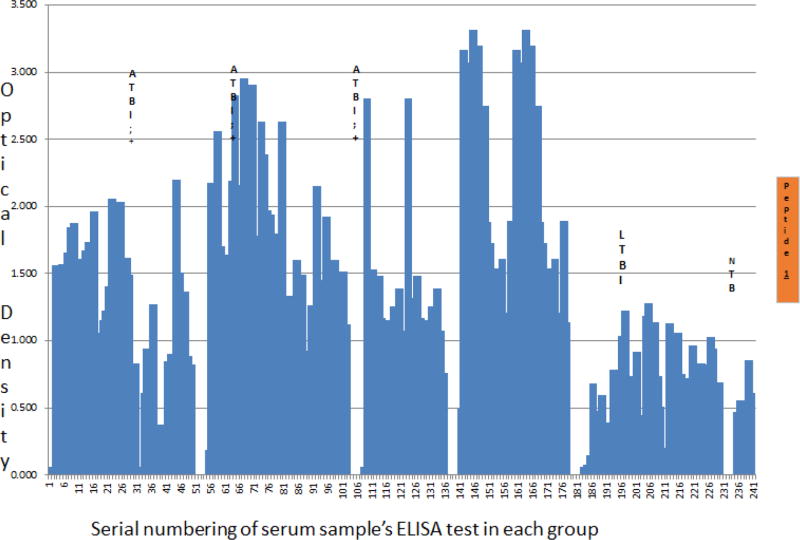
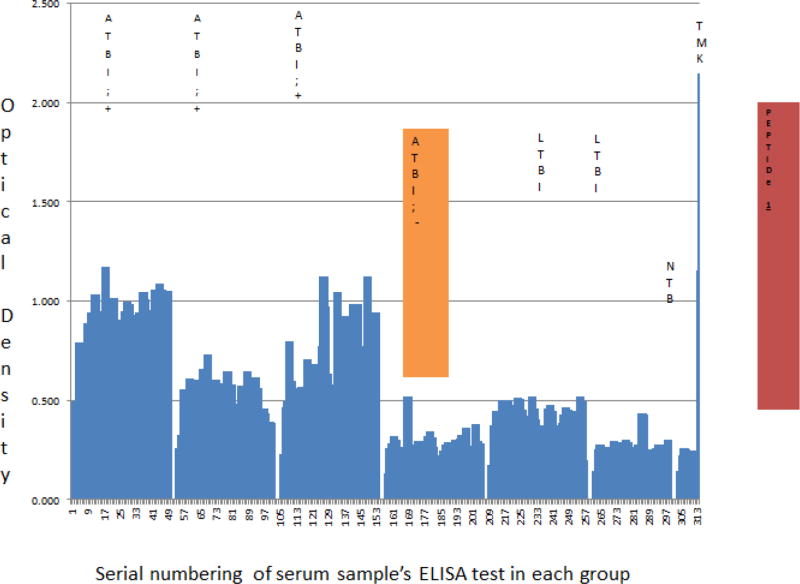
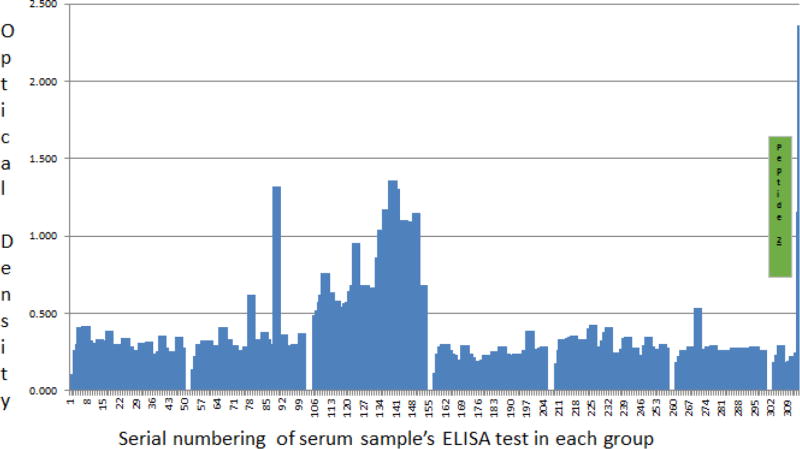
Methods and results: Direct TMKmt Ag and host specific IgG Ab detection EIAs were conducted on broadly consented, stored serum (N=281[Ag] vs. 214 [Ab] respective) samples stratified as either HIV +ve or HIV-ve ATB relative to LTBI and No TB. On one hand, UG-peptide 1 and its PAb-based EIAs accurately diagnosed ATB relative to LTBI and NTB among HIV +ve subjects {irrespectively: (a) Ag detection ATB=OD>0.490; 95% CI: 0.7446 to 0.8715 vs. LTBI=OD<0.490; 95% CI 0.4325 to 0.4829 vs. NTB=OD<0.26; 95% CI 0.1675 to 0.2567 and (b) TMKmt specific IgG detection ATB=OD>1.00; 95% CI 1.170 to 1.528 [HIV +ve] and 2.044 to 2.978 [HIV -ve] respectively vs. LTBI=OD<1.00; 95% CI 0.2690 to 0.6396 vs. NTB=OD<; 95% CI 0.1527 to 0.8751}. HIV -ve ATB presented with Ag levels greater than NTB and less than LTBI (i.e. ATB -ve=<0.490 ODs>0.26), but displayed better ant-TMKmt IgG responses (OD>2.00; 95% CI 2.044 to 2.978) relative to HIV +ve ATB (OD<1.600; 95% CI 1.170 to 1.528); suggesting a better control of M. tuberculosis-septicemia. On the other hand, UG-peptide 2 and its PAb-based EIAs did not demonstrate ATB diagnostic potential regardless of HIV sero-status, except towards designating NTB.
Conclusions: TMKmt Ab and Ag detecting EIAs based on UG-peptide 1 and its derivative PAb can accurately demarcate ATB from LTBI and NTB among HIV +ve subjects.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


