Ratko M Lasica, Jovan P Perunicic, Dejana R Popovic, Igor B Mrdovic, Ross A Arena, Nebojsa L Radovanovic, Mina R Radosavljevic-Radovanovic, Lazar D Djukanovic, Milika R Asanin
{"title":"Early and Late Mortality Predictors in Patients with Acute Aortic Dissection Type B.","authors":"Ratko M Lasica, Jovan P Perunicic, Dejana R Popovic, Igor B Mrdovic, Ross A Arena, Nebojsa L Radovanovic, Mina R Radosavljevic-Radovanovic, Lazar D Djukanovic, Milika R Asanin","doi":"10.1155/2022/7869356","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>Despite technological advances in diagnosis and treatment, in-hospital mortality with acute aortic dissection type B is still about 11%. The purpose of this study was to assess the risk factors for early and long-term adverse outcomes in patients with acute aortic dissection type B treated medically or with conventional open surgery.</p><p><strong>Methods: </strong>The present study included 104 consecutive patients with acute aortic dissection type B treated in our Center from January 1<sup>st</sup>, 1998 to January 1<sup>st</sup>, 2007. Patient demographic and clinical characteristics as well as in-hospital complications were reviewed. Univariate and multivariate testing was performed to identify the predictors of in-hospital (30-day) and late (within 9 years) mortality.</p><p><strong>Results: </strong>92 (88.5%) patients were treated medically, while 12 (11.5%) patients with complicated acute aortic dissection type B were treated by open surgical repair. In-hospital complications occurred in 35.7% patients, the most often being acute renal failure (28%), hypotension/shock (24%), mesenteric ischemia (12%), and limb ischemia (8%). The in-hospital mortality rate was 15.7% and the 9-year mortality rate was 51.9%. Independent predictors of early mortality in patients with acute aortic dissection type B were uncontrolled hypertension (HR-20.69) and a dissecting aorta diameter >4.75 cm (HR-6.30). Independent predictors of late mortality were relapsing pain (HR-7.93), uncontrolled hypertension (HR-7.25), and a pathologic difference in arterial blood pressure (>20 mmHg) (HR-5.33).</p><p><strong>Conclusion: </strong>Knowledge of key risk factors may help with a better choice of treatment and mortality reduction in acute aortic dissection type B patients.</p>","PeriodicalId":9494,"journal":{"name":"Cardiology Research and Practice","volume":" ","pages":"7869356"},"PeriodicalIF":1.8000,"publicationDate":"2022-11-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9719417/pdf/","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research and Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2022/7869356","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 5
Abstract
Background/aim: Despite technological advances in diagnosis and treatment, in-hospital mortality with acute aortic dissection type B is still about 11%. The purpose of this study was to assess the risk factors for early and long-term adverse outcomes in patients with acute aortic dissection type B treated medically or with conventional open surgery.
Methods: The present study included 104 consecutive patients with acute aortic dissection type B treated in our Center from January 1st, 1998 to January 1st, 2007. Patient demographic and clinical characteristics as well as in-hospital complications were reviewed. Univariate and multivariate testing was performed to identify the predictors of in-hospital (30-day) and late (within 9 years) mortality.
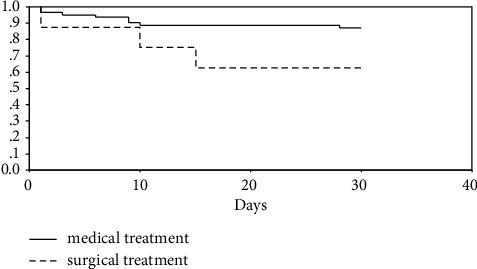
Results: 92 (88.5%) patients were treated medically, while 12 (11.5%) patients with complicated acute aortic dissection type B were treated by open surgical repair. In-hospital complications occurred in 35.7% patients, the most often being acute renal failure (28%), hypotension/shock (24%), mesenteric ischemia (12%), and limb ischemia (8%). The in-hospital mortality rate was 15.7% and the 9-year mortality rate was 51.9%. Independent predictors of early mortality in patients with acute aortic dissection type B were uncontrolled hypertension (HR-20.69) and a dissecting aorta diameter >4.75 cm (HR-6.30). Independent predictors of late mortality were relapsing pain (HR-7.93), uncontrolled hypertension (HR-7.25), and a pathologic difference in arterial blood pressure (>20 mmHg) (HR-5.33).
Conclusion: Knowledge of key risk factors may help with a better choice of treatment and mortality reduction in acute aortic dissection type B patients.
背景/目的:尽管诊断和治疗技术进步,急性B型主动脉夹层的住院死亡率仍约为11%。本研究的目的是评估药物治疗或常规开放手术治疗的急性B型主动脉夹层患者早期和长期不良结局的危险因素。方法:本研究纳入1998年1月1日至2007年1月1日在我中心连续治疗的104例急性B型主动脉夹层患者。回顾了患者人口统计学和临床特征以及院内并发症。进行单因素和多因素检验以确定住院(30天)和晚期(9年内)死亡率的预测因素。结果:92例(88.5%)患者经内科治疗,12例(11.5%)合并急性B型主动脉夹层行开放性手术修复。35.7%的患者出现院内并发症,最常见的是急性肾功能衰竭(28%)、低血压/休克(24%)、肠系膜缺血(12%)和肢体缺血(8%)。住院死亡率为15.7%,9年死亡率为51.9%。急性B型主动脉夹层患者早期死亡的独立预测因子是未控制的高血压(HR-20.69)和夹层主动脉直径>4.75 cm (HR-6.30)。晚期死亡的独立预测因子是复发性疼痛(HR-7.93)、未控制的高血压(HR-7.25)和动脉血压的病理差异(>20 mmHg) (HR-5.33)。结论:了解关键危险因素有助于更好地选择治疗方法,降低急性B型主动脉夹层患者的死亡率。
期刊介绍:
Cardiology Research and Practice is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies that focus on the diagnosis and treatment of cardiovascular disease. The journal welcomes submissions related to systemic hypertension, arrhythmia, congestive heart failure, valvular heart disease, vascular disease, congenital heart disease, and cardiomyopathy.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


