Catherine Linzay, Abhishek Seth, Kunal Suryawala, Ankur Sheth, Moheb Boktor, John Bienvenu, Robby Rahim, Guillermo P Sangster, Paul A Jordan
{"title":"The Aftermath of a Hepatic Artery Aneurysm-A Rare Etiology of Biliary Obstruction!","authors":"Catherine Linzay, Abhishek Seth, Kunal Suryawala, Ankur Sheth, Moheb Boktor, John Bienvenu, Robby Rahim, Guillermo P Sangster, Paul A Jordan","doi":"10.1177/1179552217711430","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hepatic artery aneurysms (HAAs) constitute 14% to 20% of visceral artery aneurysms. Most HAAs are asymptomatic. Although rare, obstructive jaundice due to external bile duct compression or rupture of the HAA into the biliary tree with occlusion of the lumen from blood clots has been reported.</p><p><strong>Case presentation: </strong>A 56-year-old white man presented to an outside hospital with symptoms of obstructive jaundice, including abdominal pain and yellowing of the skin. Imaging showed a large HAA. Patient was transferred to our hospital where an endoscopic retrograde cholangiopancreatography with biliary stenting was performed. This was followed by coil embolization of the HAA with improvement in symptoms and liver chemistries.</p><p><strong>Conclusions: </strong>Most clinicians agree that management of HAA is highly variable and depends on clinical presentation and anatomic location. Biliary stenting provides temporary relief for patients with obstructive jaundice. Definitive options include open aneurysmal repair versus endovascular therapy. Hepatic artery aneurysms represent a significant risk for hemorrhage and therefore must be addressed promptly once discovered.</p>","PeriodicalId":10382,"journal":{"name":"Clinical Medicine Insights. Gastroenterology","volume":"10 ","pages":"1179552217711430"},"PeriodicalIF":0.0000,"publicationDate":"2017-06-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179552217711430","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179552217711430","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
Abstract
Background: Hepatic artery aneurysms (HAAs) constitute 14% to 20% of visceral artery aneurysms. Most HAAs are asymptomatic. Although rare, obstructive jaundice due to external bile duct compression or rupture of the HAA into the biliary tree with occlusion of the lumen from blood clots has been reported.
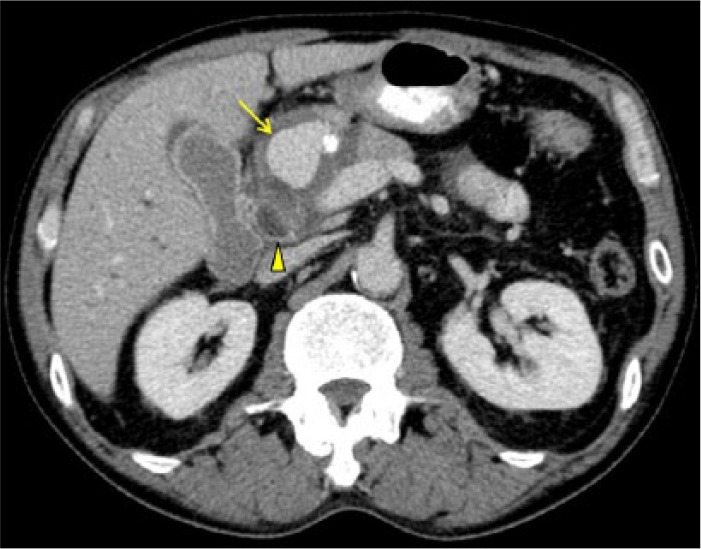
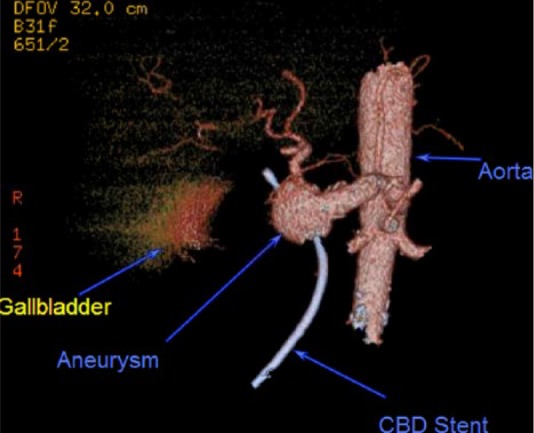
Case presentation: A 56-year-old white man presented to an outside hospital with symptoms of obstructive jaundice, including abdominal pain and yellowing of the skin. Imaging showed a large HAA. Patient was transferred to our hospital where an endoscopic retrograde cholangiopancreatography with biliary stenting was performed. This was followed by coil embolization of the HAA with improvement in symptoms and liver chemistries.
Conclusions: Most clinicians agree that management of HAA is highly variable and depends on clinical presentation and anatomic location. Biliary stenting provides temporary relief for patients with obstructive jaundice. Definitive options include open aneurysmal repair versus endovascular therapy. Hepatic artery aneurysms represent a significant risk for hemorrhage and therefore must be addressed promptly once discovered.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


