Julian We Jarman, Tina D Hunter, Wajid Hussain, Jamie L March, Tom Wong, Vias Markides
{"title":"Stroke rates before and after ablation of atrial fibrillation and in propensity-matched controls in the UK.","authors":"Julian We Jarman, Tina D Hunter, Wajid Hussain, Jamie L March, Tom Wong, Vias Markides","doi":"10.2147/POR.S134781","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We sought to determine whether catheter ablation of atrial fibrillation (AF) is associated with reduced occurrence of ischemic cerebrovascular events.</p><p><strong>Methods and results: </strong>Using routinely collected hospital data, ablation patients were matched to two control cohorts via direct and propensity score matching. A total of 4,991 ablation patients were matched 1:1 to general AF controls with no ablation, and 5,407 ablation patients were similarly matched to controls who underwent cardioversion. Yearly rates of ischemic stroke or transient ischemic attack (stroke/TIA) before and after an index date were compared between cohorts. Index date was defined as the first ablation, the first cardioversion, or the second AF event in the general AF cohort. Matched populations had very similar demographic and comorbidity profiles, including nearly identical CHA<sub>2</sub>DS<sub>2</sub>-VASc risk distribution (<i>p</i>-values 0.6948 and 0.8152 vs general AF and cardioversion cohorts). Statistical models of stroke/TIA risk in the preindex period showed no difference in annual event rates between cohorts (mean±standard error 0.30% ± 0.08% ablation vs 0.28% ± 0.07% general AF, <i>p</i>=0.8292; 0.37% ± 0.09% ablation vs 0.42% ± 0.08% cardioversion, <i>p</i>=0.5198). Postindex models showed significantly lower annual rates of stroke/TIA in ablation patients compared with each control group over 5 years (0.64% ± 0.11% ablation vs 1.84% ± 0.23% general AF, <i>p</i><0.0001; 0.82% ± 0.15% ablation vs 1.37% ± 0.18% cardioversion, <i>p</i>=0.0222).</p><p><strong>Conclusion: </strong>Matching resulted in cohorts having the same baseline risks and rates of ischemic cerebrovascular events. After the index date, there were significantly lower yearly event rates in the ablation cohort. These results suggest the divergence in outcome rates stems from variance in the treatment pathways beginning at the index date.</p>","PeriodicalId":20399,"journal":{"name":"Pragmatic and Observational Research","volume":"8 ","pages":"107-118"},"PeriodicalIF":2.3000,"publicationDate":"2017-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/POR.S134781","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pragmatic and Observational Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/POR.S134781","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 8
Abstract
Background: We sought to determine whether catheter ablation of atrial fibrillation (AF) is associated with reduced occurrence of ischemic cerebrovascular events.
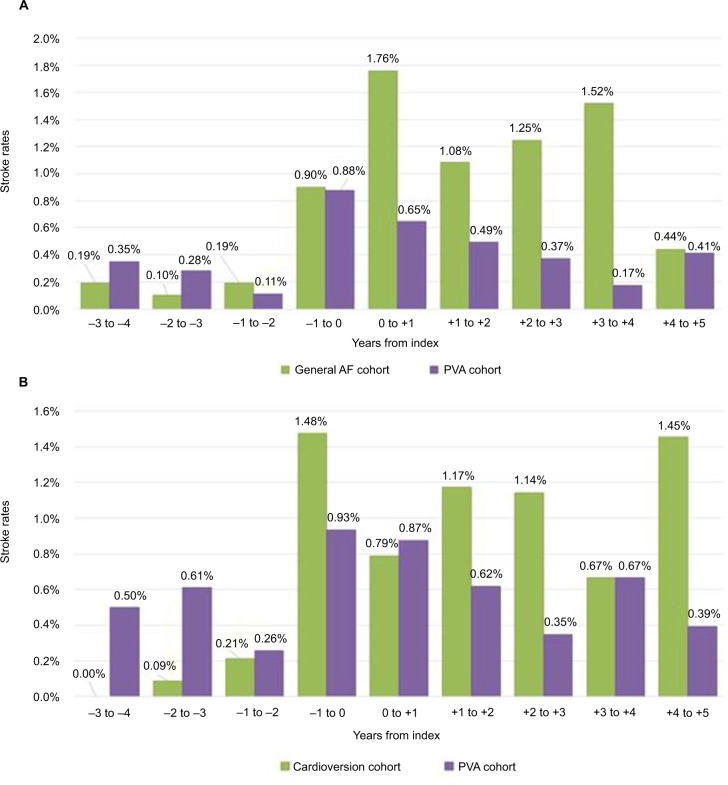
Methods and results: Using routinely collected hospital data, ablation patients were matched to two control cohorts via direct and propensity score matching. A total of 4,991 ablation patients were matched 1:1 to general AF controls with no ablation, and 5,407 ablation patients were similarly matched to controls who underwent cardioversion. Yearly rates of ischemic stroke or transient ischemic attack (stroke/TIA) before and after an index date were compared between cohorts. Index date was defined as the first ablation, the first cardioversion, or the second AF event in the general AF cohort. Matched populations had very similar demographic and comorbidity profiles, including nearly identical CHA2DS2-VASc risk distribution (p-values 0.6948 and 0.8152 vs general AF and cardioversion cohorts). Statistical models of stroke/TIA risk in the preindex period showed no difference in annual event rates between cohorts (mean±standard error 0.30% ± 0.08% ablation vs 0.28% ± 0.07% general AF, p=0.8292; 0.37% ± 0.09% ablation vs 0.42% ± 0.08% cardioversion, p=0.5198). Postindex models showed significantly lower annual rates of stroke/TIA in ablation patients compared with each control group over 5 years (0.64% ± 0.11% ablation vs 1.84% ± 0.23% general AF, p<0.0001; 0.82% ± 0.15% ablation vs 1.37% ± 0.18% cardioversion, p=0.0222).
Conclusion: Matching resulted in cohorts having the same baseline risks and rates of ischemic cerebrovascular events. After the index date, there were significantly lower yearly event rates in the ablation cohort. These results suggest the divergence in outcome rates stems from variance in the treatment pathways beginning at the index date.
期刊介绍:
Pragmatic and Observational Research is an international, peer-reviewed, open-access journal that publishes data from studies designed to closely reflect medical interventions in real-world clinical practice, providing insights beyond classical randomized controlled trials (RCTs). While RCTs maximize internal validity for cause-and-effect relationships, they often represent only specific patient groups. This journal aims to complement such studies by providing data that better mirrors real-world patients and the usage of medicines, thus informing guidelines and enhancing the applicability of research findings across diverse patient populations encountered in everyday clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


