Jaco Voorham, Bernard Vrijens, Job Fm van Boven, Dermot Ryan, Marc Miravitlles, Lisa M Law, David B Price
{"title":"Does co-payment for inhaler devices affect therapy adherence and disease outcomes? A historical, matched cohort study.","authors":"Jaco Voorham, Bernard Vrijens, Job Fm van Boven, Dermot Ryan, Marc Miravitlles, Lisa M Law, David B Price","doi":"10.2147/POR.S132658","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adherence to asthma and chronic obstructive pulmonary disease (COPD) treatment has been shown to depend on patient-level factors, such as disease severity, and medication-level factors, such as complexity. However, little is known about the impact of prescription charges - a factor at the health care system level. This study used real-life data to investigate whether co-payment affects adherence (implementation and persistence) and disease outcomes in patients with asthma or COPD.</p><p><strong>Methods: </strong>A matched, historical cohort study was carried out using two UK primary care databases. The exposure was co-payment for prescriptions, which is required for most patients in England but not in Scotland. Two comparison cohorts were formed: one comprising patients registered at general practices in England and the other comprising patients registered in Scotland. Patients aged 20-59 years with asthma, or 40-59 years with COPD, who were initiated on fluticasone propionate/salmeterol xinafoate, were included, matched to patients in the opposite cohort, and followed up for 1 year following fluticasone propionate/salmeterol xinafoate initiation. The primary outcome was good adherence, defined as medication possession ratio ≥80%, and was analyzed using conditional logistic regression. Secondary outcomes included exacerbation rate.</p><p><strong>Results: </strong>There were 1,640 patients in the payment cohort, ie, England (1,378 patients with asthma and 262 patients with COPD) and 619 patients in the no-payment cohort, ie, Scotland (512 patients with asthma and 107 patients with COPD). The proportion of patients with good adherence was 34.3% and 34.9% in the payment and no-payment cohorts, respectively, across both disease groups. In a multivariable model, no difference in odds of good adherence was found between the cohorts (odds ratio, 1.04; 95% confidence interval, 0.85-1.27). There was also no difference in exacerbation rate.</p><p><strong>Conclusion: </strong>There was no difference in adherence between matched patients registered in England and Scotland, suggesting that prescription charges do not have an impact on adherence to treatment.</p>","PeriodicalId":20399,"journal":{"name":"Pragmatic and Observational Research","volume":"8 ","pages":"31-41"},"PeriodicalIF":2.3000,"publicationDate":"2017-04-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/POR.S132658","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pragmatic and Observational Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/POR.S132658","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 4
Abstract
Background: Adherence to asthma and chronic obstructive pulmonary disease (COPD) treatment has been shown to depend on patient-level factors, such as disease severity, and medication-level factors, such as complexity. However, little is known about the impact of prescription charges - a factor at the health care system level. This study used real-life data to investigate whether co-payment affects adherence (implementation and persistence) and disease outcomes in patients with asthma or COPD.
Methods: A matched, historical cohort study was carried out using two UK primary care databases. The exposure was co-payment for prescriptions, which is required for most patients in England but not in Scotland. Two comparison cohorts were formed: one comprising patients registered at general practices in England and the other comprising patients registered in Scotland. Patients aged 20-59 years with asthma, or 40-59 years with COPD, who were initiated on fluticasone propionate/salmeterol xinafoate, were included, matched to patients in the opposite cohort, and followed up for 1 year following fluticasone propionate/salmeterol xinafoate initiation. The primary outcome was good adherence, defined as medication possession ratio ≥80%, and was analyzed using conditional logistic regression. Secondary outcomes included exacerbation rate.
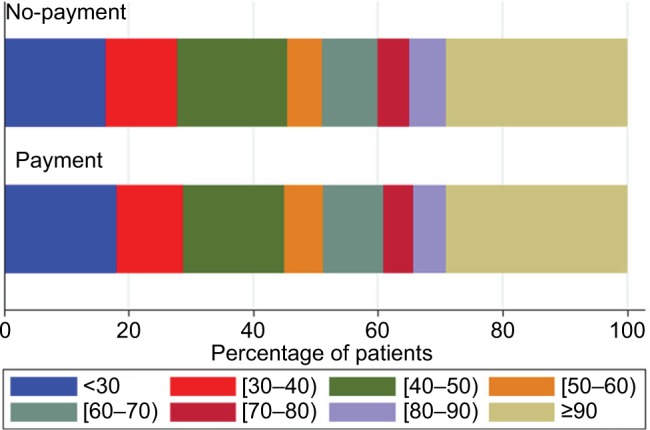
Results: There were 1,640 patients in the payment cohort, ie, England (1,378 patients with asthma and 262 patients with COPD) and 619 patients in the no-payment cohort, ie, Scotland (512 patients with asthma and 107 patients with COPD). The proportion of patients with good adherence was 34.3% and 34.9% in the payment and no-payment cohorts, respectively, across both disease groups. In a multivariable model, no difference in odds of good adherence was found between the cohorts (odds ratio, 1.04; 95% confidence interval, 0.85-1.27). There was also no difference in exacerbation rate.
Conclusion: There was no difference in adherence between matched patients registered in England and Scotland, suggesting that prescription charges do not have an impact on adherence to treatment.
期刊介绍:
Pragmatic and Observational Research is an international, peer-reviewed, open-access journal that publishes data from studies designed to closely reflect medical interventions in real-world clinical practice, providing insights beyond classical randomized controlled trials (RCTs). While RCTs maximize internal validity for cause-and-effect relationships, they often represent only specific patient groups. This journal aims to complement such studies by providing data that better mirrors real-world patients and the usage of medicines, thus informing guidelines and enhancing the applicability of research findings across diverse patient populations encountered in everyday clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


