Stephanie A Rutledge, Svetlana Masalovich, Rachel J Blacher, Magon M Saunders
{"title":"Diabetes Self-Management Education Programs in Nonmetropolitan Counties - United States, 2016.","authors":"Stephanie A Rutledge, Svetlana Masalovich, Rachel J Blacher, Magon M Saunders","doi":"10.15585/mmwr.ss6610a1","DOIUrl":null,"url":null,"abstract":"<p><strong>Problem/condition: </strong>Diabetes self-management education (DSME) is a clinical practice intended to improve preventive practices and behaviors with a focus on decision-making, problem-solving, and self-care. The distribution and correlates of established DSME programs in nonmetropolitan counties across the United States have not been previously described, nor have the characteristics of the nonmetropolitan counties with DSME programs.</p><p><strong>Reporting period: </strong>July 2016.</p><p><strong>Description of systems: </strong>DSME programs recognized by the American Diabetes Association or accredited by the American Association of Diabetes Educators (i.e., active programs) as of July 2016 were shared with CDC by both organizations. The U.S. Census Bureau's census geocoder was used to identify the county of each DSME program site using documented addresses. County characteristic data originated from the U.S. Census Bureau, compiled by the U.S. Department of Agriculture's Economic Research Service into the 2013 Atlas of Rural and Small-Town America data set. County levels of diagnosed diabetes prevalence and incidence, as well as the number of persons with diagnosed diabetes, were previously estimated by CDC. This report defined nonmetropolitan counties using the rural-urban continuum code from the 2013 Atlas of Rural and Small-Town America data set. This code included six nonmetropolitan categories of 1,976 urban and rural counties (62% of counties) adjacent to and nonadjacent to metropolitan counties.</p><p><strong>Results: </strong>In 2016, a total of 1,065 DSME programs were located in 38% of the 1,976 nonmetropolitan counties; 62% of nonmetropolitan counties did not have a DSME program. The total number of DSME programs for nonmetropolitan counties with at least one DSME program ranged from 1 to 8, with an average of 1.4 programs. After adjusting for county-level characteristics, the odds of a nonmetropolitan county having at least one DSME program increased as the percentage insured increased (adjusted odds ratio [AOR] = 1.10, 95% confidence interval [CI] = 1.08-1.13), the percentage with a high school education or less decreased (AOR = 1.06, 95% CI = 1.04-1.07), the unemployment rate decreased (AOR = 1.19, 95% CI = 1.11-1.23), and the natural logarithm of the number of persons with diabetes increased (AOR = 3.63, 95% CI = 3.15-4.19).</p><p><strong>Interpretation: </strong>In 2016, there were few DMSE programs in nonmetropolitan, socially disadvantaged counties in the United States. The number of persons with diabetes, percentage insured, percentage with a high school education or less, and the percentage unemployed were significantly associated with whether a DSME program was located in a nonmetropolitan county.</p><p><strong>Public health action: </strong>Monitoring the distribution of DSME programs at the county level provides insight needed to strategically address rural disparities in diabetes care and outcomes. These findings provide information needed to assess lack of availability of DSME programs and to explore evidence-based strategies and innovative technologies to deliver DSME programs in underserved rural communities.</p>","PeriodicalId":48549,"journal":{"name":"Mmwr Surveillance Summaries","volume":"66 10","pages":"1-6"},"PeriodicalIF":37.3000,"publicationDate":"2017-04-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5829897/pdf/","citationCount":"40","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mmwr Surveillance Summaries","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.15585/mmwr.ss6610a1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 40
Abstract
Problem/condition: Diabetes self-management education (DSME) is a clinical practice intended to improve preventive practices and behaviors with a focus on decision-making, problem-solving, and self-care. The distribution and correlates of established DSME programs in nonmetropolitan counties across the United States have not been previously described, nor have the characteristics of the nonmetropolitan counties with DSME programs.
Reporting period: July 2016.
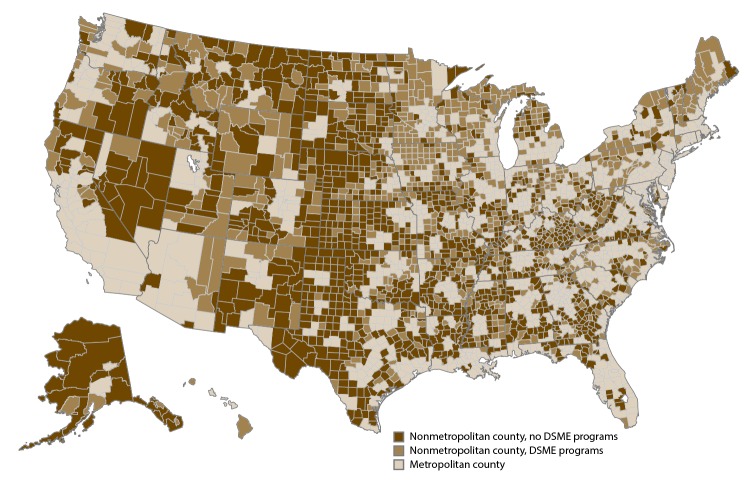
Description of systems: DSME programs recognized by the American Diabetes Association or accredited by the American Association of Diabetes Educators (i.e., active programs) as of July 2016 were shared with CDC by both organizations. The U.S. Census Bureau's census geocoder was used to identify the county of each DSME program site using documented addresses. County characteristic data originated from the U.S. Census Bureau, compiled by the U.S. Department of Agriculture's Economic Research Service into the 2013 Atlas of Rural and Small-Town America data set. County levels of diagnosed diabetes prevalence and incidence, as well as the number of persons with diagnosed diabetes, were previously estimated by CDC. This report defined nonmetropolitan counties using the rural-urban continuum code from the 2013 Atlas of Rural and Small-Town America data set. This code included six nonmetropolitan categories of 1,976 urban and rural counties (62% of counties) adjacent to and nonadjacent to metropolitan counties.
Results: In 2016, a total of 1,065 DSME programs were located in 38% of the 1,976 nonmetropolitan counties; 62% of nonmetropolitan counties did not have a DSME program. The total number of DSME programs for nonmetropolitan counties with at least one DSME program ranged from 1 to 8, with an average of 1.4 programs. After adjusting for county-level characteristics, the odds of a nonmetropolitan county having at least one DSME program increased as the percentage insured increased (adjusted odds ratio [AOR] = 1.10, 95% confidence interval [CI] = 1.08-1.13), the percentage with a high school education or less decreased (AOR = 1.06, 95% CI = 1.04-1.07), the unemployment rate decreased (AOR = 1.19, 95% CI = 1.11-1.23), and the natural logarithm of the number of persons with diabetes increased (AOR = 3.63, 95% CI = 3.15-4.19).
Interpretation: In 2016, there were few DMSE programs in nonmetropolitan, socially disadvantaged counties in the United States. The number of persons with diabetes, percentage insured, percentage with a high school education or less, and the percentage unemployed were significantly associated with whether a DSME program was located in a nonmetropolitan county.
Public health action: Monitoring the distribution of DSME programs at the county level provides insight needed to strategically address rural disparities in diabetes care and outcomes. These findings provide information needed to assess lack of availability of DSME programs and to explore evidence-based strategies and innovative technologies to deliver DSME programs in underserved rural communities.
期刊介绍:
The Morbidity and Mortality Weekly Report (MMWR) Series, produced by the Centers for Disease Control and Prevention (CDC), is commonly referred to as "the voice of CDC." Serving as the primary outlet for timely, reliable, authoritative, accurate, objective, and practical public health information and recommendations, the MMWR is a crucial publication. Its readership primarily includes physicians, nurses, public health practitioners, epidemiologists, scientists, researchers, educators, and laboratorians.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


