Quadricuspid Aortic Valve Complicated with Severe Aortic Regurgitation and Left-Sided Inferior Vena Cava.
Journal of cardiovascular ultrasound
Pub Date : 2017-03-01
Epub Date: 2017-03-27
DOI:10.4250/jcu.2017.25.1.34
引用次数: 1
Abstract
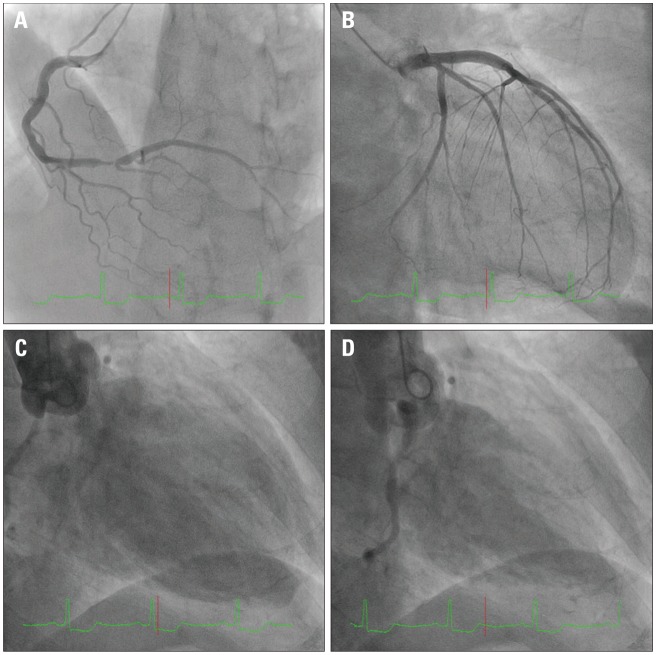
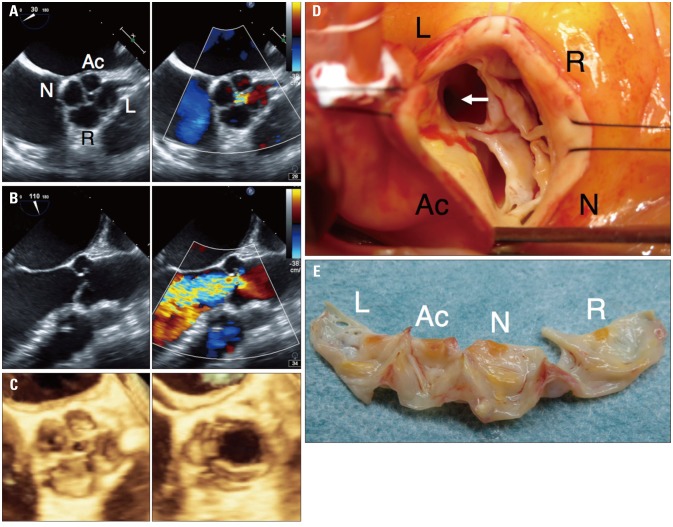
A 72-year-old man with hypertension was referred to our hospital for severe aortic regurgitation probably associated with quadricuspid aortic valve on transthoracic echocardiography. He felt general fatigue on effort. On physical examination, blood pressure was 166/54 mm Hg and cardiac auscultation indicated a systolic murmur at the aortic area together with a diastolic murmur at the left parasternal border. Value of brain natriuretic peptide was 258.5 pg/mL, and values of cardiac enzymes were within normal limits. An electrocardiogram showed left ventricular high voltage in addition to STsegment depression in II, III, aVF, and V6 leads. Subsequent transthoracic echocardiography revealed decreased motion in the inferoposterior wall of the dilated left ventricle (end-diastolic and end-systolic diameters of 6.3 and 4.6 cm, respectively; ejection fraction 49 %, Simpson’s method) and severe aortic regurgitation (vena contracta 6.7 mm, pressure half time 279 msec, regurgitant volume 77 mL on the proximal isovelocity surface area method, and effective regurgitant orifice area 0.38 cm) with probable quadricuspid aortic valve. Twoand three-dimensional transesophageal echocardiography clearly depicted a quadricuspid asymmetric aortic valve with a large right coronary cusp, two intermediate cusps including left coronary cusp and non-coronary cusp, and a smaller accessory cusp (Hurwitz and Roberts’ classification, type D), and a severe aortic regurgitation due to the central coaptation defect (Fig. 1A, B, and C, Supplementary movie 1, 2, and 3). Pre-operative cardiac catheterization was performed (Fig. 2). Coronary angiography showed a severe stenosis in the distal segment of the pISSN 1975-4612 / eISSN 2005-9655 Copyright © 2017 Korean Society of Echocardiography www.kse-jcu.org https://doi.org/10.4250/jcu.2017.25.1.34
四尖瓣主动脉瓣合并严重主动脉瓣返流及左侧下腔静脉。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


