{"title":"Role of Quantitative Wall Motion Analysis in Patients with Acute Chest Pain at Emergency Department.","authors":"Kyung-Hee Kim, Sang-Hoon Na, Jin-Sik Park","doi":"10.4250/jcu.2017.25.1.20","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Evaluation of acute chest pain in emergency department (ED), using limited resource and time, is still very difficult despite recent development of many diagnostic tools. In this study, we tried to determine the applicability of new semi-automated cardiac function analysis tool, velocity vector imaging (VVI), in the evaluation of the patients with acute chest pain in ED.</p><p><strong>Methods: </strong>We prospectively enrolled 48 patients, who visited ED with acute chest pain, and store images to analyze VVI from July 2005 to July 2007.</p><p><strong>Results: </strong>In 677 of 768 segments (88%), the analysis by VVI was feasible among 48 patients. Peak systolic radial velocity (V<sub>peak</sub>) and strain significantly decreased according to visual regional wall motion abnormality (V<sub>peak</sub>, 3.50 ± 1.34 cm/s for normal vs. 3.46 ± 1.52 cm/s for hypokinesia, 2.51 ± 1.26 for akinesia, <i>p</i> < 0.01; peak systolic radial strain -31.74 ± 9.15% fornormal, -24.33 ± 6.28% for hypokinesia, -20.30 ± 7.78% for akinesia, <i>p</i> < 0.01). However, the velocity vectors at the time of mitral valve opening (MVO) were directed outward in the visually normal myocardium, inward velocity vectors were revealed in the visually akinetic area (V<sub>MVO</sub>, -0.85 ± 1.65 cm/s for normal vs. 0.10 ± 1.46 cm/s for akinesia, <i>p</i> < 0.001). At coronary angiography, V<sub>MVO</sub> clearly increased in the ischemic area (V<sub>MVO</sub>, -0.88+1.56 cm/s for normal vs. 0.70 + 2.04 cm/s for ischemic area, <i>p</i> < 0.01).</p><p><strong>Conclusion: </strong>Regional wall motion assessment using VVI showed could be used to detect significant ischemia in the patient with acute chest pain at ED.</p>","PeriodicalId":88913,"journal":{"name":"Journal of cardiovascular ultrasound","volume":"25 1","pages":"20-27"},"PeriodicalIF":0.0000,"publicationDate":"2017-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4250/jcu.2017.25.1.20","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiovascular ultrasound","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4250/jcu.2017.25.1.20","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/3/27 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
Abstract
Background: Evaluation of acute chest pain in emergency department (ED), using limited resource and time, is still very difficult despite recent development of many diagnostic tools. In this study, we tried to determine the applicability of new semi-automated cardiac function analysis tool, velocity vector imaging (VVI), in the evaluation of the patients with acute chest pain in ED.
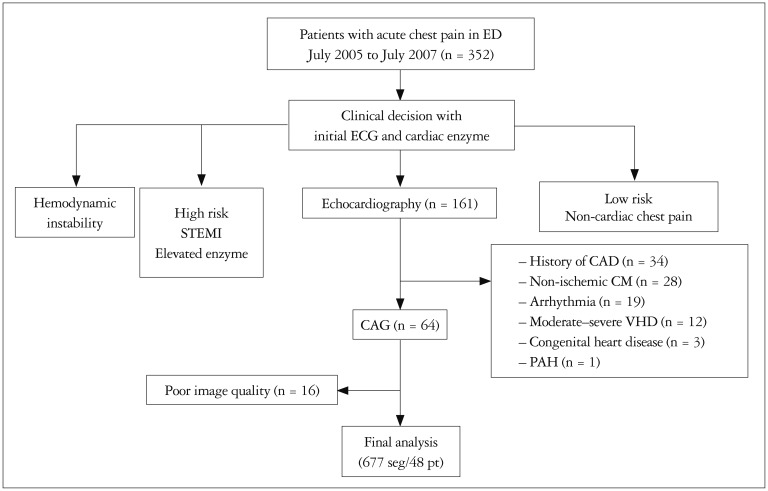
Methods: We prospectively enrolled 48 patients, who visited ED with acute chest pain, and store images to analyze VVI from July 2005 to July 2007.
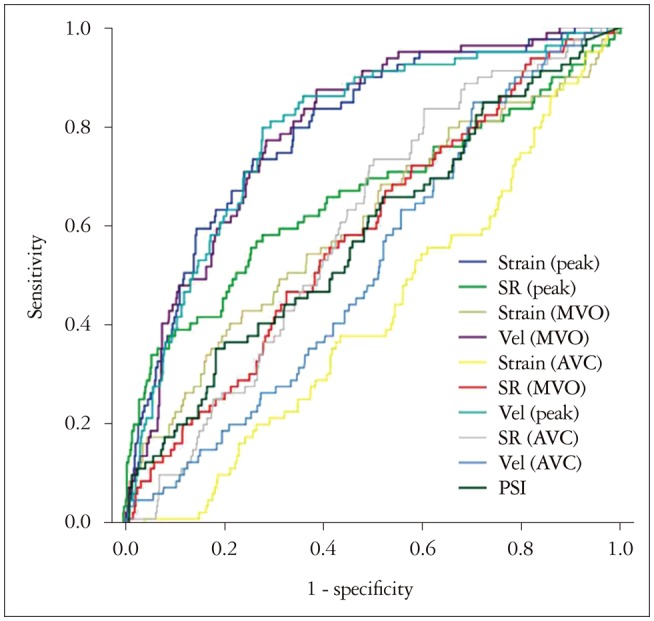
Results: In 677 of 768 segments (88%), the analysis by VVI was feasible among 48 patients. Peak systolic radial velocity (Vpeak) and strain significantly decreased according to visual regional wall motion abnormality (Vpeak, 3.50 ± 1.34 cm/s for normal vs. 3.46 ± 1.52 cm/s for hypokinesia, 2.51 ± 1.26 for akinesia, p < 0.01; peak systolic radial strain -31.74 ± 9.15% fornormal, -24.33 ± 6.28% for hypokinesia, -20.30 ± 7.78% for akinesia, p < 0.01). However, the velocity vectors at the time of mitral valve opening (MVO) were directed outward in the visually normal myocardium, inward velocity vectors were revealed in the visually akinetic area (VMVO, -0.85 ± 1.65 cm/s for normal vs. 0.10 ± 1.46 cm/s for akinesia, p < 0.001). At coronary angiography, VMVO clearly increased in the ischemic area (VMVO, -0.88+1.56 cm/s for normal vs. 0.70 + 2.04 cm/s for ischemic area, p < 0.01).
Conclusion: Regional wall motion assessment using VVI showed could be used to detect significant ischemia in the patient with acute chest pain at ED.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


