Francisco Elano Carvalho Pereira, Irene Lopes Mello, Fernando Heladio de Oliveira Medeiros Pimenta, Debora Maia Costa, Deysi Viviana Tenazoa Wong, Claudia Regina Fernandes, Roberto César Lima Junior, Josenília M Alves Gomes
{"title":"A Clinical Experimental Model to Evaluate Analgesic Effect of Remote Ischemic Preconditioning in Acute Postoperative Pain.","authors":"Francisco Elano Carvalho Pereira, Irene Lopes Mello, Fernando Heladio de Oliveira Medeiros Pimenta, Debora Maia Costa, Deysi Viviana Tenazoa Wong, Claudia Regina Fernandes, Roberto César Lima Junior, Josenília M Alves Gomes","doi":"10.1155/2016/5093870","DOIUrl":null,"url":null,"abstract":"<p><p>This study aims to evaluate the viability of a clinical model of remote ischemic preconditioning (RIPC) and its analgesic effects. It is a prospective study with twenty (20) patients randomly divided into two groups: control group and RIPC group. The opioid analgesics consumption in the postoperative period, the presence of secondary mechanical hyperalgesia, the scores of postoperative pain by visual analog scale, and the plasma levels interleukins (IL-6) were evaluated. The tourniquet applying after spinal anesthetic block was safe, producing no pain for all patients in the tourniquet group. The total dose of morphine consumption in 24 hours was significantly lower in RIPC group than in the control group (p = 0.0156). The intensity analysis of rest pain, pain during coughing and pain in deep breathing, showed that visual analogue scale (VAS) scores were significantly lower in RIPC group compared to the control group: p = 0.0087, 0.0119, and 0.0015, respectively. There were no differences between groups in the analysis of presence or absence of mechanical hyperalgesia (p = 0.0704) and in the serum levels of IL-6 dosage over time (p < 0.0001). This clinical model of remote ischemic preconditioning promoted satisfactory analgesia in patients undergoing conventional cholecystectomy, without changing serum levels of IL-6. </p>","PeriodicalId":19786,"journal":{"name":"Pain Research and Treatment","volume":"2016 ","pages":"5093870"},"PeriodicalIF":0.0000,"publicationDate":"2016-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2016/5093870","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pain Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2016/5093870","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/6/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 8
Abstract
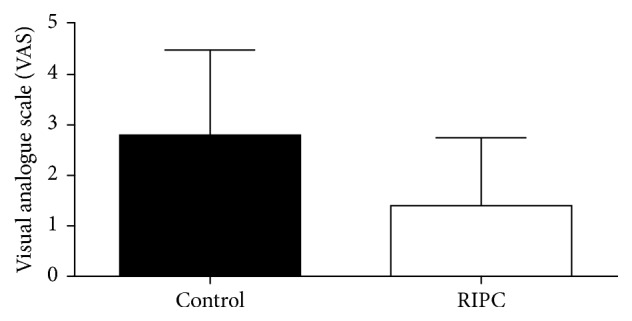
This study aims to evaluate the viability of a clinical model of remote ischemic preconditioning (RIPC) and its analgesic effects. It is a prospective study with twenty (20) patients randomly divided into two groups: control group and RIPC group. The opioid analgesics consumption in the postoperative period, the presence of secondary mechanical hyperalgesia, the scores of postoperative pain by visual analog scale, and the plasma levels interleukins (IL-6) were evaluated. The tourniquet applying after spinal anesthetic block was safe, producing no pain for all patients in the tourniquet group. The total dose of morphine consumption in 24 hours was significantly lower in RIPC group than in the control group (p = 0.0156). The intensity analysis of rest pain, pain during coughing and pain in deep breathing, showed that visual analogue scale (VAS) scores were significantly lower in RIPC group compared to the control group: p = 0.0087, 0.0119, and 0.0015, respectively. There were no differences between groups in the analysis of presence or absence of mechanical hyperalgesia (p = 0.0704) and in the serum levels of IL-6 dosage over time (p < 0.0001). This clinical model of remote ischemic preconditioning promoted satisfactory analgesia in patients undergoing conventional cholecystectomy, without changing serum levels of IL-6.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


