{"title":"Circulating Levels of M30 and M65 Molecules in Transitional Cell Carcinoma of the Bladder and Their Relation to Tumor Progression.","authors":"Zahra Malek-Hosseini, Abdolaziz Khezri, Zahra Amirghofran","doi":"10.17795/ijcp-4086","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Various markers are suggested for diagnosis and monitoring of transitional cell carcinoma of the bladder (TCC), including cytokeratins (CKs).</p><p><strong>Objectives: </strong>In the present study, the circulating CK18 (M65) and its caspase-cleaved form, ccCK18 (M30), have been investigated in a group of patients with TCC.</p><p><strong>Patients and methods: </strong>Serum samples were obtained from 60 patients before surgical resection, among which the samples of 26 patients after resection were also included. We measured the levels of soluble M30 and M65 molecules by enzyme-linked immunosorbent assay. The relation between these markers and patients' clinical characteristics was evaluated.</p><p><strong>Results: </strong>M30 and M65 in total patient sera were 148 ± 16 U/L and 318 ± 34 U/L, respectively. A correlation existed between pre-operative M30 and M65 levels (P < 0.0001, Spearman r = 0.51). M65, but not M30, showed a significant relation to tumor stage and grade. The M65 quantity in patients with T3/T4 tumor stages (350 ± 42 U/L) was higher than that of patients with T1/T2 stages (293 ± 45U/L; P < 0.038). Patients with tumor grades III/IV also showed higher levels of M65 compared to patients with tumor grades I/II (P < 0.04). The M30:M65 ratio in all patients was 0.54 ± 0.04. There was a lower M30:M65 ratio in patients with T3/T4 stage tumors and those with tumor grades III/IV (P < 0.02). The M30 (133 ± 19 U/L) and M65 levels (240 ± 21 U/L) after surgery did not significantly differ compared to their pre-operative values. However, a correlation between the pre- and post-operative M30:M65 ratio in patients ≥ 70 years was seen (P = 0.009).</p><p><strong>Conclusions: </strong>These data suggested a relationship of both M65 and the M30:M65 ratio to tumor progression which might imply their importance in TCC monitoring.</p>","PeriodicalId":73510,"journal":{"name":"Iranian journal of cancer prevention","volume":"9 2","pages":"e4086"},"PeriodicalIF":0.0000,"publicationDate":"2016-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0d/61/ijcp-09-02-4086.PMC4951759.pdf","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Iranian journal of cancer prevention","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17795/ijcp-4086","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 6
Abstract
Background: Various markers are suggested for diagnosis and monitoring of transitional cell carcinoma of the bladder (TCC), including cytokeratins (CKs).
Objectives: In the present study, the circulating CK18 (M65) and its caspase-cleaved form, ccCK18 (M30), have been investigated in a group of patients with TCC.
Patients and methods: Serum samples were obtained from 60 patients before surgical resection, among which the samples of 26 patients after resection were also included. We measured the levels of soluble M30 and M65 molecules by enzyme-linked immunosorbent assay. The relation between these markers and patients' clinical characteristics was evaluated.
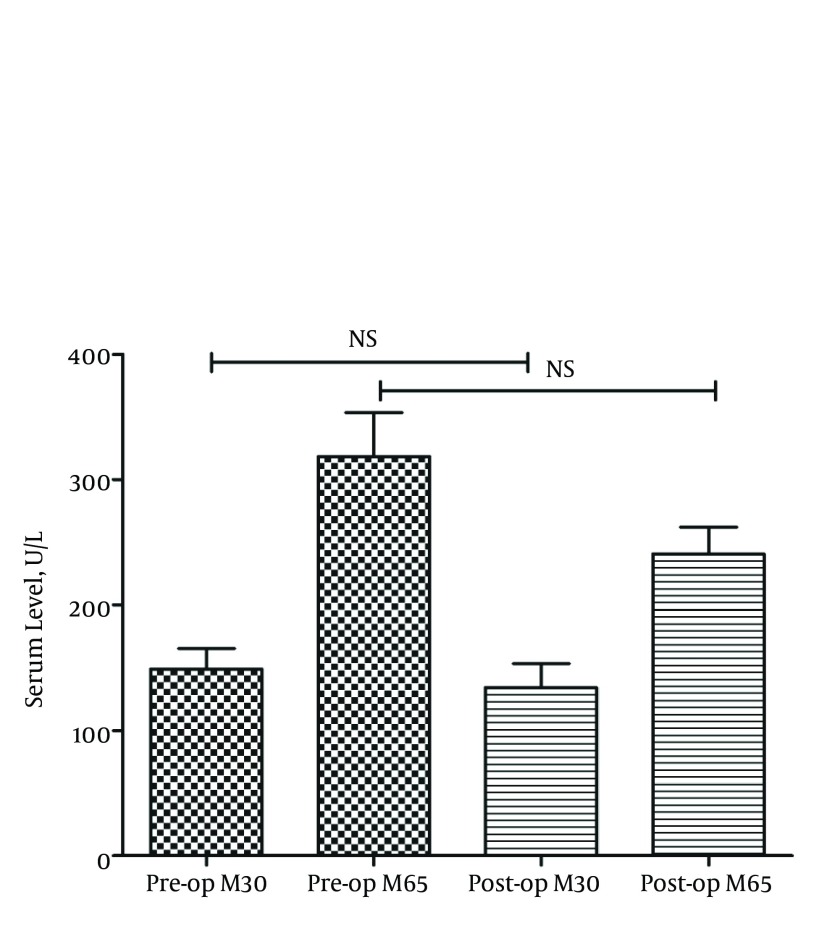
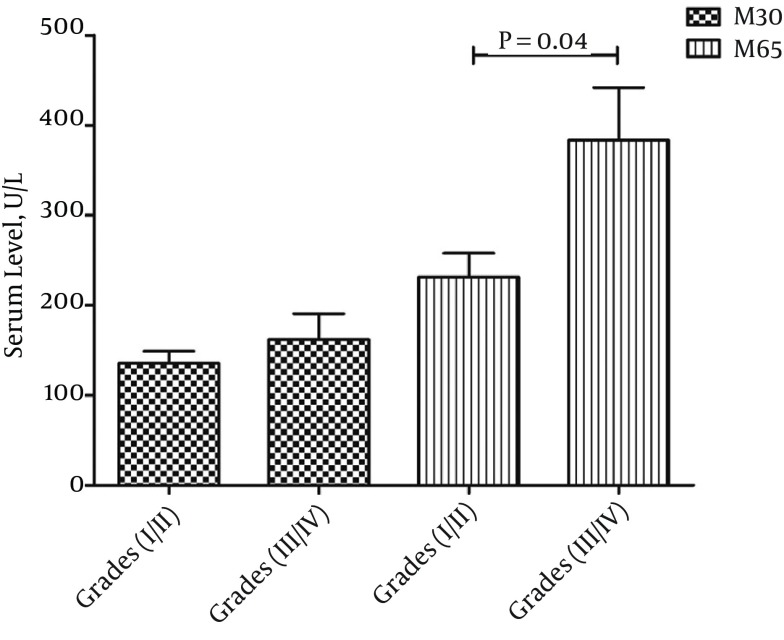
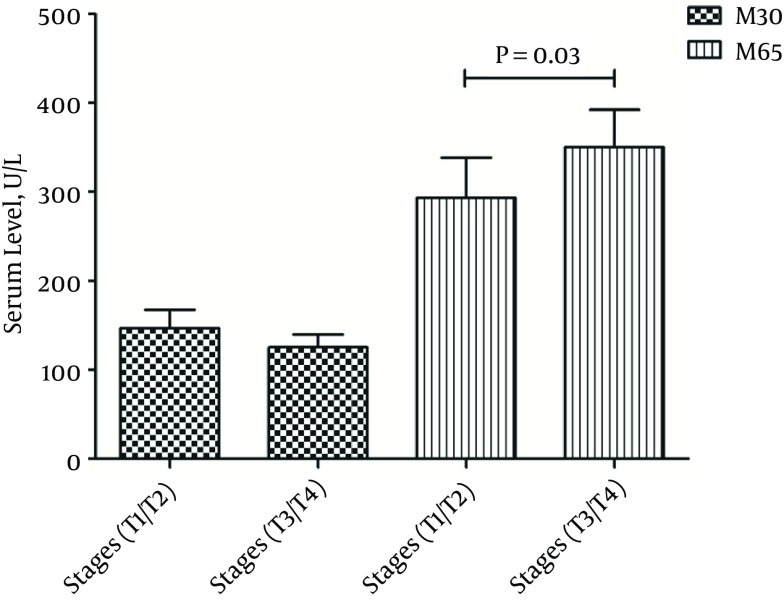
Results: M30 and M65 in total patient sera were 148 ± 16 U/L and 318 ± 34 U/L, respectively. A correlation existed between pre-operative M30 and M65 levels (P < 0.0001, Spearman r = 0.51). M65, but not M30, showed a significant relation to tumor stage and grade. The M65 quantity in patients with T3/T4 tumor stages (350 ± 42 U/L) was higher than that of patients with T1/T2 stages (293 ± 45U/L; P < 0.038). Patients with tumor grades III/IV also showed higher levels of M65 compared to patients with tumor grades I/II (P < 0.04). The M30:M65 ratio in all patients was 0.54 ± 0.04. There was a lower M30:M65 ratio in patients with T3/T4 stage tumors and those with tumor grades III/IV (P < 0.02). The M30 (133 ± 19 U/L) and M65 levels (240 ± 21 U/L) after surgery did not significantly differ compared to their pre-operative values. However, a correlation between the pre- and post-operative M30:M65 ratio in patients ≥ 70 years was seen (P = 0.009).
Conclusions: These data suggested a relationship of both M65 and the M30:M65 ratio to tumor progression which might imply their importance in TCC monitoring.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


