B Mbwele, A Slot, Q De Mast, P Kweka, M Msuya, M Hulscher
{"title":"The Use of Guidelines for Lower Respiratory Tract Infections in Tanzania: A Lesson from Kilimanjaro Clinicians.","authors":"B Mbwele, A Slot, Q De Mast, P Kweka, M Msuya, M Hulscher","doi":"10.4103/2141-9248.181845","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Evaluations of the guidelines for the management of Lower Respiratory Tract Infections (LRTI) Sub-Saharan Africa, particularly in Tanzania is scant.</p><p><strong>Aim: </strong>The aim of the study was to assess the usefulness of the current Tanzanian treatment guideline for the management lower respiratory tract infection.</p><p><strong>Subjects and methods: </strong>A descriptive cross sectional study in 11 hospitals of different levels in the Kilimanjaro region Data were collected from May 2012 to July 2012 by semi-structured interview for clinicians using 2 dummy cases for practical assessment. Data were analyzed by STATA v11 (StataCorp, TX, USA). Qualitative narratives from the interviews were translated, transcribed then coded by colors into meaningful themes.</p><p><strong>Results: </strong>A variety of principles for diagnosing and managing LRTI were demonstrated by 53 clinicians of Kilimanjaro. For the awareness, 67.9% (36/53) clinicians knew their responsibility to use Standard Treatment Guideline for managing LRTI. The content derived from Standard Treatment Guideline could be cited by 11.3% of clinicians (6/53) however they all showed concern of gaps in the guideline. Previous training in the management of patients with LRTI was reported by 25.9% (14/53), majority were pulmonary TB related. Correct microorganisms causing different forms of LRTI were mentioned by 11.3% (6/53). Exact cause of Atypical pneumonia and Q fever as an example was stated by 13.0% (7/53) from whom the need of developing the guideline for LRTI was explicitly elaborated.</p><p><strong>Conclusion: </strong>The current guidelines have not been used effectively for the management of LRTI in Tanzania. There is a need to review its content for the current practical use.</p>","PeriodicalId":8186,"journal":{"name":"Annals of Medical and Health Sciences Research","volume":"6 2","pages":"100-8"},"PeriodicalIF":0.0000,"publicationDate":"2016-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8b/f3/AMHSR-6-100.PMC4866362.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Medical and Health Sciences Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/2141-9248.181845","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
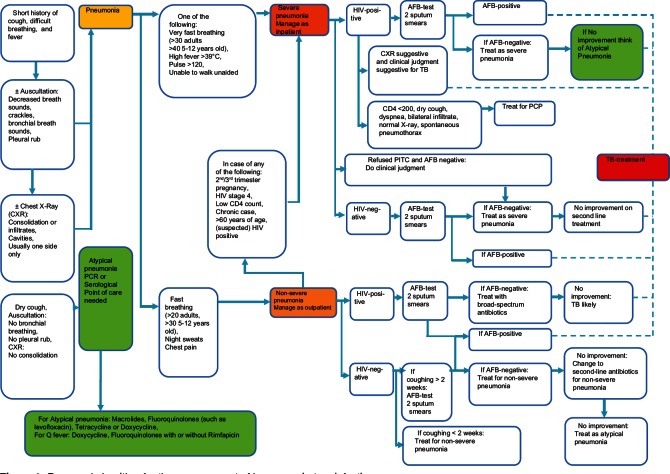
Background: Evaluations of the guidelines for the management of Lower Respiratory Tract Infections (LRTI) Sub-Saharan Africa, particularly in Tanzania is scant.
Aim: The aim of the study was to assess the usefulness of the current Tanzanian treatment guideline for the management lower respiratory tract infection.
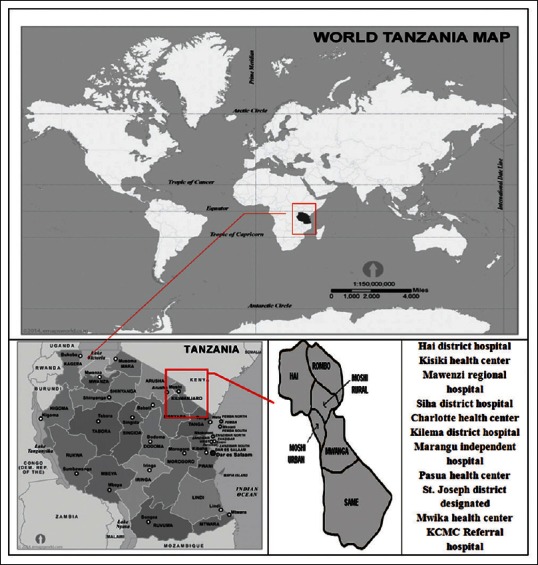
Subjects and methods: A descriptive cross sectional study in 11 hospitals of different levels in the Kilimanjaro region Data were collected from May 2012 to July 2012 by semi-structured interview for clinicians using 2 dummy cases for practical assessment. Data were analyzed by STATA v11 (StataCorp, TX, USA). Qualitative narratives from the interviews were translated, transcribed then coded by colors into meaningful themes.
Results: A variety of principles for diagnosing and managing LRTI were demonstrated by 53 clinicians of Kilimanjaro. For the awareness, 67.9% (36/53) clinicians knew their responsibility to use Standard Treatment Guideline for managing LRTI. The content derived from Standard Treatment Guideline could be cited by 11.3% of clinicians (6/53) however they all showed concern of gaps in the guideline. Previous training in the management of patients with LRTI was reported by 25.9% (14/53), majority were pulmonary TB related. Correct microorganisms causing different forms of LRTI were mentioned by 11.3% (6/53). Exact cause of Atypical pneumonia and Q fever as an example was stated by 13.0% (7/53) from whom the need of developing the guideline for LRTI was explicitly elaborated.
Conclusion: The current guidelines have not been used effectively for the management of LRTI in Tanzania. There is a need to review its content for the current practical use.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


