{"title":"Decrement of mirror movements by repetitive transcranial magnetic stimulation in a patient with porencephaly.","authors":"Sung H Jang, Hyeok G Kwon","doi":"10.17712/nsj.2016.2.20150674","DOIUrl":null,"url":null,"abstract":"M movements (MM) are involuntary movements which occur on one side of the body as a mirror reversal of the intentional movement on the other side of the body. Mirror movements, which are normally observed during early childhood, decrease with development of the brain, and then usually disappear around the end of the first decade of life. Persistence of MM in adulthood is considered pathological and can be seen in various congenital brain disorders. Severe MM of the hands can hinder the activities of daily living which require bilateral hand coordination. However, little is known on the management modality of MM.1,2 The pathogenetic mechanism of MM has not been clearly elucidated; however, the most plausible mechanism is the ipsilateral motor pathway, which involves from the unaffected motor cortex to the affected limb based on the inhibition hypothesis.3 Many studies have demonstrated the safety and effectiveness of repetitive transcranial magnetic stimulation (rTMS) for suppressing the unaffected motor cortex in stroke patients. In addition, a recent study demonstrated the cessation of MM and deactivation of the unaffected motor cortex by rTMS for 2 weeks in a patient with a cerebral infarct.2 Regarding MM in patients with a congenital brain lesion, one study reported that rTMS for 2 weeks resulted in relief of MM in a patient with congenital MM.1 However, no functional neuroimaging study on the effect of rTMS on the unaffected motor cortex in a patient with a congenital brain lesion has been reported. In this study, we report on a patient with porencephaly in whom the intensity of MM and activation of the unaffected motor cortex were decreased after application of rTMS, as evaluated by functional magnetic resonance imaging (fMRI). A 21-year-old male patient had exhibited left hemiparesis since birth. He was delivered at full-term without complications. He was diagnosed as a congenital porencephalic cyst in the right frontal area and underwent shunt operation at 6 months after birth. He complained of severe MM, and as a result, performing bimanual activities such as typing is difficult. He signed an informed consent statement, and the study protocol was approved by the Institutional Review Board of a university hospital. Frameless stereotaxic neuronavigation (TMSNavigator, Localite, Sankt Augustin, Germany) based on the coregistered patient’s T1-weighted image was used for navigation of the TMS coil and to maintain its precise location and orientation throughout TMS sessions. The patient underwent 10 sessions of rTMS performed to the activation area of the primary sensorimotor cortex (SM1) in the left hemisphere on fMRI, according to the following protocol: frequency 1 Hz, intensity of motor threshold 100%, 1200 stimuli as a single, continuous train lasting 5 minutes, for 5 sessions per week for a period of 2 weeks. Mirror movements were evaluated according to the degree of involuntary movement of the unaffected hand during performance of a functional MRI task using the modified MM scale by Woods and Teuber (1978).4 The Purdue Pegboard test was used for evaluation of hand dexterity of both hands. Blood oxygenation level dependent (BOLD) fMRI measurements were performed 2 times (prerTMS and post-rTMS after 2 weeks), using a 1.5-T. Using a block paradigm (21s control, 21s stimulation: 3 cycles), hand grasp-release movements (1Hz) were performed for stimulation. SPM 8 software (Wellcome Department of Cognitive Neurology, London, UK) running in the MATLAB environment (The Mathworks, Natick, Mass., USA) was used for analysis of fMRI data. For changes in BOLD signal, the control condition data were subtracted from the stimulated condition data. Statistical parametric maps were obtained, and voxels of cluster level were considered significant at a threshold of uncorrected p<0.001. On pre-rTMS fMRI, movement of fingers on one hand resulted in a grade 4 MM of the fingers of the opposite hand (the movement range of the metacarpophalangeal (MP) joint: the right hand50°, and the left hand60°). By contrast, on post-rTMS fMRI, movement of fingers on one hand on the first fMRI resulted in a grade 3 MM of the fingers of the opposite hand (the movement range of the MP joint: the right hand10°, and the left hand20°). The Purdue Pegboard score (PPC) for both hands was increased after rTMS (the right handfrom 14 to 16, and the left handfrom 2 to 4). On Disclosure. This work was funded by the Korea government National Research Fund grant no 2015R1D1A4A01020385.","PeriodicalId":520723,"journal":{"name":"Neurosciences (Riyadh, Saudi Arabia)","volume":" ","pages":"170-2"},"PeriodicalIF":1.3000,"publicationDate":"2016-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9e/ba/Neurosciences-21-170.PMC5107275.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurosciences (Riyadh, Saudi Arabia)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.17712/nsj.2016.2.20150674","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
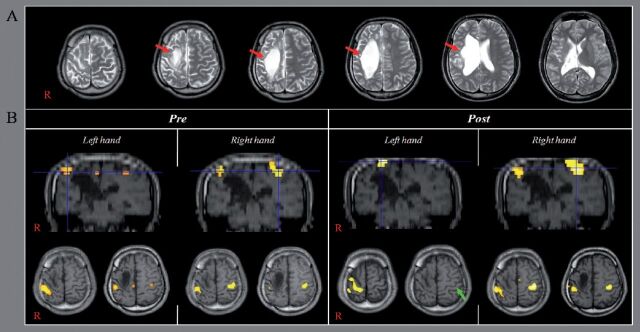
M movements (MM) are involuntary movements which occur on one side of the body as a mirror reversal of the intentional movement on the other side of the body. Mirror movements, which are normally observed during early childhood, decrease with development of the brain, and then usually disappear around the end of the first decade of life. Persistence of MM in adulthood is considered pathological and can be seen in various congenital brain disorders. Severe MM of the hands can hinder the activities of daily living which require bilateral hand coordination. However, little is known on the management modality of MM.1,2 The pathogenetic mechanism of MM has not been clearly elucidated; however, the most plausible mechanism is the ipsilateral motor pathway, which involves from the unaffected motor cortex to the affected limb based on the inhibition hypothesis.3 Many studies have demonstrated the safety and effectiveness of repetitive transcranial magnetic stimulation (rTMS) for suppressing the unaffected motor cortex in stroke patients. In addition, a recent study demonstrated the cessation of MM and deactivation of the unaffected motor cortex by rTMS for 2 weeks in a patient with a cerebral infarct.2 Regarding MM in patients with a congenital brain lesion, one study reported that rTMS for 2 weeks resulted in relief of MM in a patient with congenital MM.1 However, no functional neuroimaging study on the effect of rTMS on the unaffected motor cortex in a patient with a congenital brain lesion has been reported. In this study, we report on a patient with porencephaly in whom the intensity of MM and activation of the unaffected motor cortex were decreased after application of rTMS, as evaluated by functional magnetic resonance imaging (fMRI). A 21-year-old male patient had exhibited left hemiparesis since birth. He was delivered at full-term without complications. He was diagnosed as a congenital porencephalic cyst in the right frontal area and underwent shunt operation at 6 months after birth. He complained of severe MM, and as a result, performing bimanual activities such as typing is difficult. He signed an informed consent statement, and the study protocol was approved by the Institutional Review Board of a university hospital. Frameless stereotaxic neuronavigation (TMSNavigator, Localite, Sankt Augustin, Germany) based on the coregistered patient’s T1-weighted image was used for navigation of the TMS coil and to maintain its precise location and orientation throughout TMS sessions. The patient underwent 10 sessions of rTMS performed to the activation area of the primary sensorimotor cortex (SM1) in the left hemisphere on fMRI, according to the following protocol: frequency 1 Hz, intensity of motor threshold 100%, 1200 stimuli as a single, continuous train lasting 5 minutes, for 5 sessions per week for a period of 2 weeks. Mirror movements were evaluated according to the degree of involuntary movement of the unaffected hand during performance of a functional MRI task using the modified MM scale by Woods and Teuber (1978).4 The Purdue Pegboard test was used for evaluation of hand dexterity of both hands. Blood oxygenation level dependent (BOLD) fMRI measurements were performed 2 times (prerTMS and post-rTMS after 2 weeks), using a 1.5-T. Using a block paradigm (21s control, 21s stimulation: 3 cycles), hand grasp-release movements (1Hz) were performed for stimulation. SPM 8 software (Wellcome Department of Cognitive Neurology, London, UK) running in the MATLAB environment (The Mathworks, Natick, Mass., USA) was used for analysis of fMRI data. For changes in BOLD signal, the control condition data were subtracted from the stimulated condition data. Statistical parametric maps were obtained, and voxels of cluster level were considered significant at a threshold of uncorrected p<0.001. On pre-rTMS fMRI, movement of fingers on one hand resulted in a grade 4 MM of the fingers of the opposite hand (the movement range of the metacarpophalangeal (MP) joint: the right hand50°, and the left hand60°). By contrast, on post-rTMS fMRI, movement of fingers on one hand on the first fMRI resulted in a grade 3 MM of the fingers of the opposite hand (the movement range of the MP joint: the right hand10°, and the left hand20°). The Purdue Pegboard score (PPC) for both hands was increased after rTMS (the right handfrom 14 to 16, and the left handfrom 2 to 4). On Disclosure. This work was funded by the Korea government National Research Fund grant no 2015R1D1A4A01020385.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


