Isaac O Abah, Victor B Ojeh, Kakjing D Falang, Kristin M Darin, Oluremi O Olaitan, Oche O Agbaji
{"title":"Pharmaceutical care outcomes in an outpatient human immunodeficiency virus treatment center in Jos, Nigeria.","authors":"Isaac O Abah, Victor B Ojeh, Kakjing D Falang, Kristin M Darin, Oluremi O Olaitan, Oche O Agbaji","doi":"10.4103/0976-0105.139727","DOIUrl":null,"url":null,"abstract":"<p><strong>Rationale: </strong>Pharmacotherapy for patients infected with human immunodeficiency virus (HIV) is complex and increases the potential for drug therapy problems (DTPs). We described the frequency and type of DTPs in a Nigerian cohort of HIV infected patients on antiretroviral therapy (ART), as well as the changes in HIV clinical outcomes after pharmacists' intervention.</p><p><strong>Methods: </strong>A prospective 1-year descriptive study was conducted from July 2010 to June 2011, at the adult HIV clinic of Jos University Teaching Hospital, Nigeria. DTPs and the associated pharmacist-initiated interventions were documented. Chi-square and Wilcoxon signed ranks test was used as appropriate, to compare the main outcome measures of pre- and post-intervention levels of viral load and CD+ cell count.</p><p><strong>Results: </strong>A total of 64,839 prescriptions were dispensed to 9320 patients. Interventions were documented for 85 unique patients (incidence of 1.31 interventions/1000 prescriptions), of which 62 (73%) and 3 (3.5%) were on first- and second-line ART, respectively, while 20 (23.5%) were yet to commence ART. Reasons for pharmacist intervention included failure to initiate therapy for HIV or hepatitis B infection; therapeutic failure (25.9%); and drug toxicity (24.7%). After intervention, the percentage of patients with HIV ribonucleic acid level <400 copies/mL rose from 29.4% to 67.1% (P < 0.001), while median (interquartile range) CD4+ cell count increased from 200 (123-351) to 361 (221-470) cells/mm(3) (P < 0.001).</p><p><strong>Conclusion: </strong>Pharmacist intervention resulted in clinically significant improvements in patients HIV virological and immunological outcomes. This highlights an important role for the pharmacist in the treatment and care of HIV-infected patients, in a multidisciplinary team.</p>","PeriodicalId":15046,"journal":{"name":"Journal of Basic and Clinical Pharmacy","volume":"5 3","pages":"57-61"},"PeriodicalIF":0.0000,"publicationDate":"2014-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0f/c1/JBCP-5-57.PMC4160720.pdf","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Basic and Clinical Pharmacy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/0976-0105.139727","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 7
Abstract
Rationale: Pharmacotherapy for patients infected with human immunodeficiency virus (HIV) is complex and increases the potential for drug therapy problems (DTPs). We described the frequency and type of DTPs in a Nigerian cohort of HIV infected patients on antiretroviral therapy (ART), as well as the changes in HIV clinical outcomes after pharmacists' intervention.
Methods: A prospective 1-year descriptive study was conducted from July 2010 to June 2011, at the adult HIV clinic of Jos University Teaching Hospital, Nigeria. DTPs and the associated pharmacist-initiated interventions were documented. Chi-square and Wilcoxon signed ranks test was used as appropriate, to compare the main outcome measures of pre- and post-intervention levels of viral load and CD+ cell count.
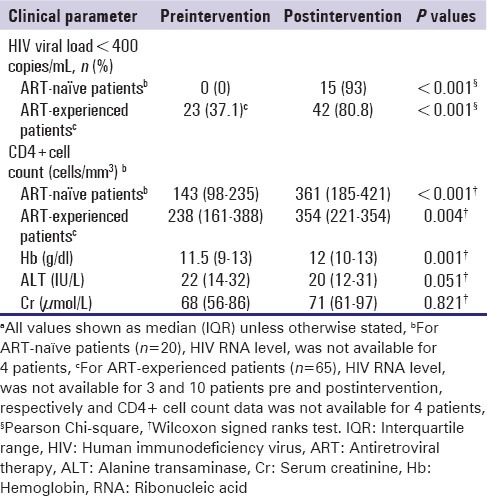
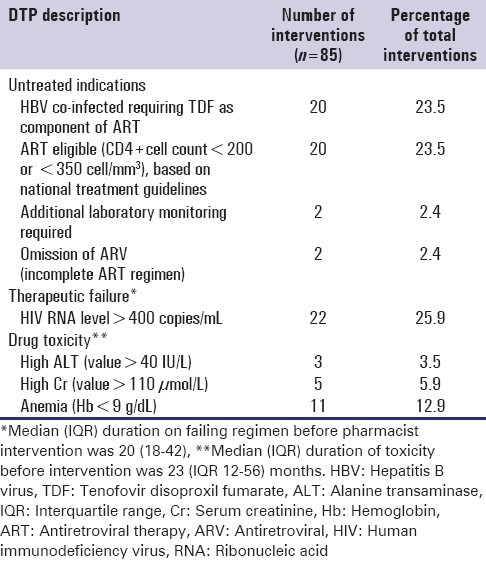
Results: A total of 64,839 prescriptions were dispensed to 9320 patients. Interventions were documented for 85 unique patients (incidence of 1.31 interventions/1000 prescriptions), of which 62 (73%) and 3 (3.5%) were on first- and second-line ART, respectively, while 20 (23.5%) were yet to commence ART. Reasons for pharmacist intervention included failure to initiate therapy for HIV or hepatitis B infection; therapeutic failure (25.9%); and drug toxicity (24.7%). After intervention, the percentage of patients with HIV ribonucleic acid level <400 copies/mL rose from 29.4% to 67.1% (P < 0.001), while median (interquartile range) CD4+ cell count increased from 200 (123-351) to 361 (221-470) cells/mm(3) (P < 0.001).
Conclusion: Pharmacist intervention resulted in clinically significant improvements in patients HIV virological and immunological outcomes. This highlights an important role for the pharmacist in the treatment and care of HIV-infected patients, in a multidisciplinary team.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


