Heterotopic pancreas in omphalomesenteric duct remnant results in persistent umbilical discharge.
Korean Journal of Pathology
Pub Date : 2014-08-01
Epub Date: 2014-08-26
DOI:10.4132/KoreanJPathol.2014.48.4.323
引用次数: 13
Abstract
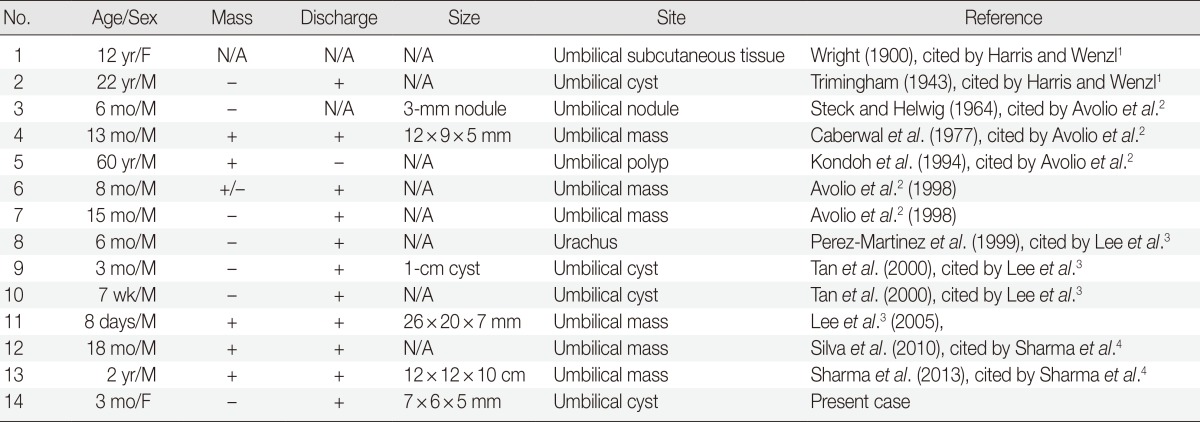
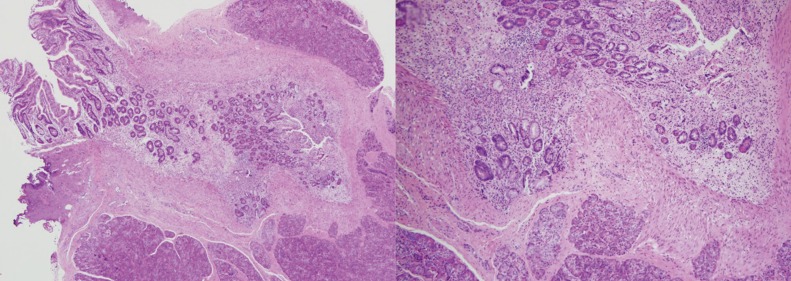
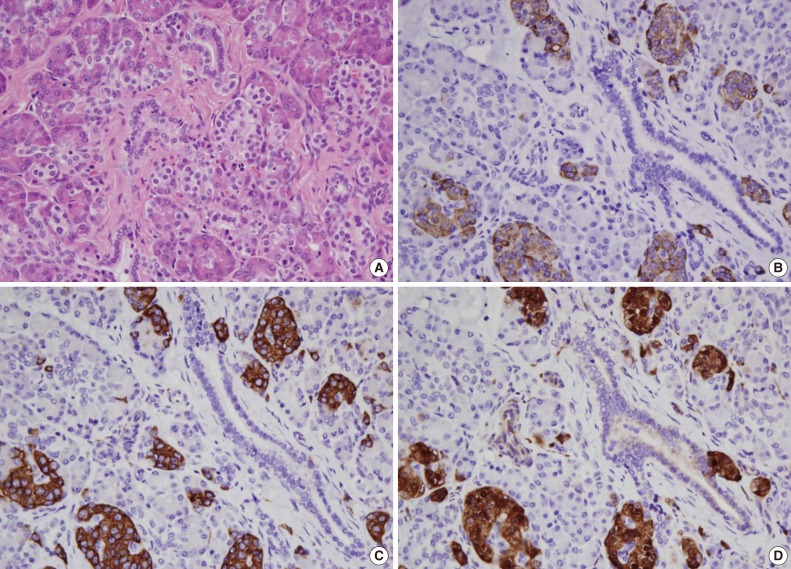
Umbilical discharge in infancy is a common pediatric problem and usually attributed to infection or an umbilical granuloma. However, it is important to investigate if such discharge is due to an underlying congenital abnormality such as umbilical hernia ulceration, urachal remnant, or omphalomesenteric duct remnant, because corrective surgical intervention may then be required. Omphalomesenteric duct remnant can cause umbilical discharge generally through patency between the gut and umbilicus. However, though rare, umbilical discharge may be due to the presence of heterotopic pancreas. The prevalence of omphalomesenteric duct remnant is only 2% of the population, and most of them remain asymptomatic. The present case is an infant with persistent umbilical discharge caused by heterotopic pancreatic tissue in a remnant omphalomesenteric duct. To the best of our knowledge, this is the first such case report in Korea. A 3-month-old female infant presented with persistent umbilical discharge since birth. The infant was born through normal vaginal delivery following an uneventful gestational period and had no congenital anomalies. She had been gaining weight well and had no family history of genitourinary or gastrointestinal problems. Ultrasonography of the abdomen revealed an isoechoic tract posterior to the umbilicus, and the diagnosis of urachal remnant was suspected. On physical examination, small droplets of clear fluid constantly discharged from a normallooking umbilicus. Laboratory examination results were within normal limits. Under general anesthesia, an incision was made below umbilicus. Surgical exploration showed a fibrous sinus posterior to the umbilicus which was attached to the inner aspect of the umbilicus and the outer wall of the ileum by a fi brous band. Fibrous tissue was excised close to both ends, and the rest was ligated by suture tie. The excised specimen was a 7×6×5-mm-sized whitish fibrous tissue. Histologically, the excised specimen included pancreatic tissue with some small intestinal mucosa and fibrous extracellular components (Fig. 1). Both exocrine and endocrine pancreatic tissues were observed, including acini, ducts, and islets of Langerhans. Acini were separated into lobules by connective tissue. Intercalated ducts were lined by simple low cuboidal epithelium (Fig. 2). The patient was discharged without any postoperative complications and is currently alive without any sequelae.
脐肠系管残余的异位胰腺导致持续的脐带放电。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


