Current Concepts and Occurrence of Epithelial Odontogenic Tumors: II. Calcifying Epithelial Odontogenic Tumor Versus Ghost Cell Odontogenic Tumors Derived from Calcifying Odontogenic Cyst.
{"title":"Current Concepts and Occurrence of Epithelial Odontogenic Tumors: II. Calcifying Epithelial Odontogenic Tumor Versus Ghost Cell Odontogenic Tumors Derived from Calcifying Odontogenic Cyst.","authors":"Suk Keun Lee, Yeon Sook Kim","doi":"10.4132/KoreanJPathol.2014.48.3.175","DOIUrl":null,"url":null,"abstract":"<p><p>Calcifying epithelial odontogenic tumors (CEOTs) and ghost cell odontogenic tumors (GCOTs) are characteristic odontogenic origin epithelial tumors which produce calcifying materials from transformed epithelial tumor cells. CEOT is a benign odontogenic tumor composed of polygonal epithelial tumor cells that show retrogressive calcific changes, amyloid-like deposition, and clear cytoplasm. Differentially, GCOTs are a group of transient tumors characterized by ghost cell presence, which comprise calcifying cystic odontogenic tumor (CCOT), dentinogenic ghost cell tumor (DGCT), and ghost cell odontogenic carcinoma (GCOC), all derived from calcifying odontogenic cysts (COCs). There is considerable confusion about COCs and GCOTs terminology, but these lesions can be classified as COCs or GCOTs, based on their cystic or tumorous natures, respectively. GCOTs include ameloblastomatous tumors derived from dominant odontogenic cysts classified as CCOTs, ghost cell-rich tumors producing dentinoid materials as DGCTs, and the GCOT malignant counterpart, GCOCs. Many authors have reported CEOTs and GCOTs variably express keratins, β-catenin, BCL-2, BSP, RANKL, OPG, Notch1, Jagged1, TGF-β, SMADs, and other proteins. However, these heterogeneous lesions should be differentially diagnosed to allow for accurate tumor progression and prognosis prediction. </p>","PeriodicalId":49936,"journal":{"name":"Korean Journal of Pathology","volume":"48 3","pages":"175-87"},"PeriodicalIF":0.0000,"publicationDate":"2014-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4132/KoreanJPathol.2014.48.3.175","citationCount":"40","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Pathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4132/KoreanJPathol.2014.48.3.175","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/6/26 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 40
Abstract
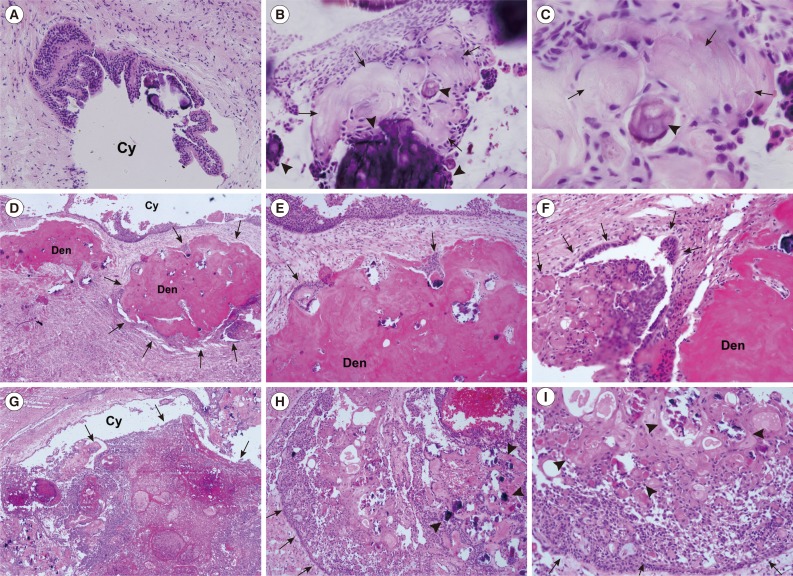
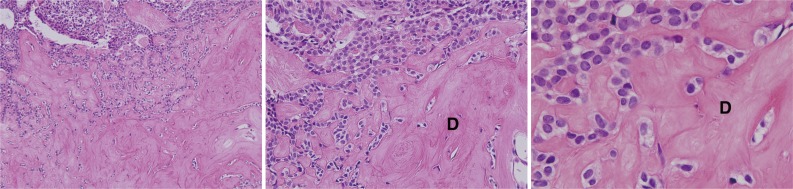
Calcifying epithelial odontogenic tumors (CEOTs) and ghost cell odontogenic tumors (GCOTs) are characteristic odontogenic origin epithelial tumors which produce calcifying materials from transformed epithelial tumor cells. CEOT is a benign odontogenic tumor composed of polygonal epithelial tumor cells that show retrogressive calcific changes, amyloid-like deposition, and clear cytoplasm. Differentially, GCOTs are a group of transient tumors characterized by ghost cell presence, which comprise calcifying cystic odontogenic tumor (CCOT), dentinogenic ghost cell tumor (DGCT), and ghost cell odontogenic carcinoma (GCOC), all derived from calcifying odontogenic cysts (COCs). There is considerable confusion about COCs and GCOTs terminology, but these lesions can be classified as COCs or GCOTs, based on their cystic or tumorous natures, respectively. GCOTs include ameloblastomatous tumors derived from dominant odontogenic cysts classified as CCOTs, ghost cell-rich tumors producing dentinoid materials as DGCTs, and the GCOT malignant counterpart, GCOCs. Many authors have reported CEOTs and GCOTs variably express keratins, β-catenin, BCL-2, BSP, RANKL, OPG, Notch1, Jagged1, TGF-β, SMADs, and other proteins. However, these heterogeneous lesions should be differentially diagnosed to allow for accurate tumor progression and prognosis prediction.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


