Allison Steigler, James W Denham, David S Lamb, Nigel A Spry, David Joseph, John Matthews, Chris Atkinson, Sandra Turner, John North, David Christie, Keen-Hun Tai, Chris Wynne
{"title":"Risk Stratification after Biochemical Failure following Curative Treatment of Locally Advanced Prostate Cancer: Data from the TROG 96.01 Trial.","authors":"Allison Steigler, James W Denham, David S Lamb, Nigel A Spry, David Joseph, John Matthews, Chris Atkinson, Sandra Turner, John North, David Christie, Keen-Hun Tai, Chris Wynne","doi":"10.1155/2012/814724","DOIUrl":null,"url":null,"abstract":"<p><p>Purpose. Survival following biochemical failure is highly variable. Using a randomized trial dataset, we sought to define a risk stratification scheme in men with locally advanced prostate cancer (LAPC). Methods. The TROG 96.01 trial randomized 802 men with LAPC to radiation ± neoadjuvant androgen suppression therapy (AST) between 1996 and 2000. Ten-year follow-up data was used to develop three-tier post-biochemical failure risk stratification schemes based on cutpoints of time to biochemical failure (TTBF) and PSA doubling time (PSADT). Schemes were evaluated in univariable, competing risk models for prostate cancer-specific mortality. The performance was assessed by c-indices and internally validated by the simple bootstrap method. Performance rankings were compared in sensitivity analyses using multivariable models and variations in PSADT calculation. Results. 485 men developed biochemical failure. c-indices ranged between 0.630 and 0.730. The most discriminatory scheme had a high risk category defined by PSADT < 4 months or TTBF < 1 year and low risk category by PSADT > 9 months or TTBF > 3 years. Conclusion. TTBF and PSADT can be combined to define risk stratification schemes after biochemical failure in men with LAPC treated with short-term AST and radiotherapy. External validation, particularly in long-term AST and radiotherapy datasets, is necessary.</p>","PeriodicalId":20907,"journal":{"name":"Prostate Cancer","volume":"2012 ","pages":"814724"},"PeriodicalIF":2.3000,"publicationDate":"2012-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2012/814724","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Prostate Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2012/814724","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/12/24 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 7
Abstract
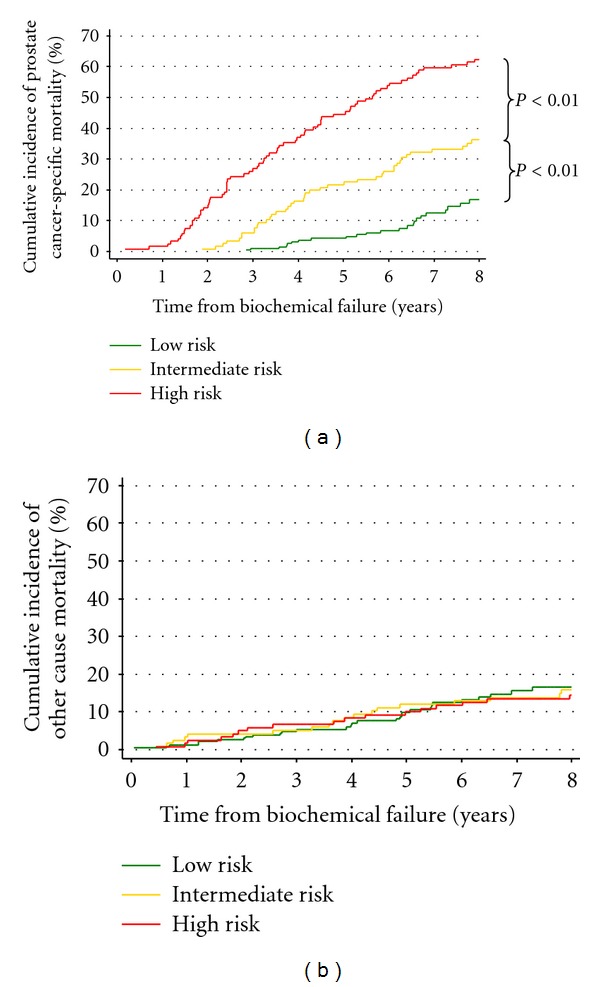
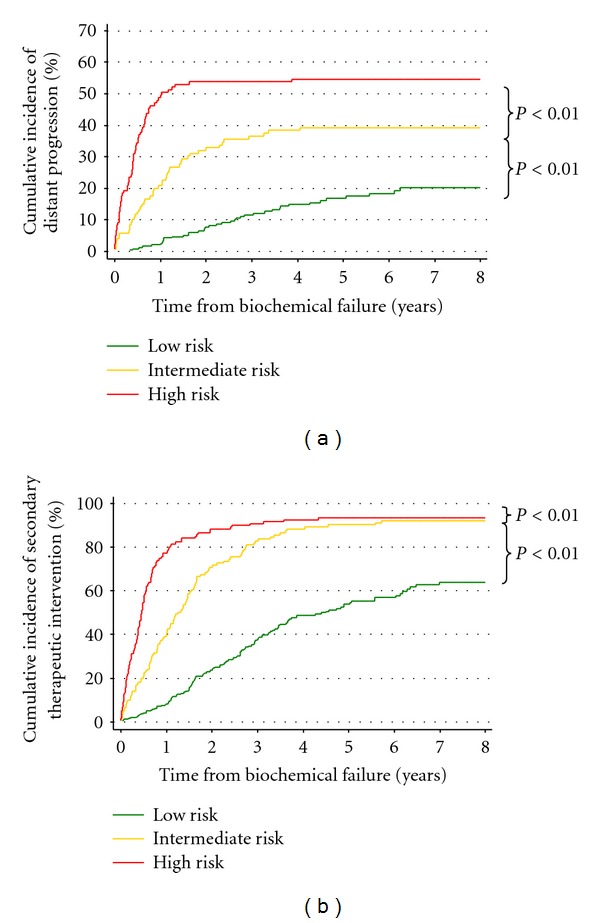
Purpose. Survival following biochemical failure is highly variable. Using a randomized trial dataset, we sought to define a risk stratification scheme in men with locally advanced prostate cancer (LAPC). Methods. The TROG 96.01 trial randomized 802 men with LAPC to radiation ± neoadjuvant androgen suppression therapy (AST) between 1996 and 2000. Ten-year follow-up data was used to develop three-tier post-biochemical failure risk stratification schemes based on cutpoints of time to biochemical failure (TTBF) and PSA doubling time (PSADT). Schemes were evaluated in univariable, competing risk models for prostate cancer-specific mortality. The performance was assessed by c-indices and internally validated by the simple bootstrap method. Performance rankings were compared in sensitivity analyses using multivariable models and variations in PSADT calculation. Results. 485 men developed biochemical failure. c-indices ranged between 0.630 and 0.730. The most discriminatory scheme had a high risk category defined by PSADT < 4 months or TTBF < 1 year and low risk category by PSADT > 9 months or TTBF > 3 years. Conclusion. TTBF and PSADT can be combined to define risk stratification schemes after biochemical failure in men with LAPC treated with short-term AST and radiotherapy. External validation, particularly in long-term AST and radiotherapy datasets, is necessary.
期刊介绍:
Prostate Cancer is a peer-reviewed, Open Access journal that provides a multidisciplinary platform for scientists, surgeons, oncologists and clinicians working on prostate cancer. The journal publishes original research articles, review articles, and clinical studies related to the diagnosis, surgery, radiotherapy, drug discovery and medical management of the disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


