Chuan Luo, Deepa Ramachandran, David L Ware, Tony S Ma, John W Clark
{"title":"Modeling left ventricular diastolic dysfunction: classification and key indicators.","authors":"Chuan Luo, Deepa Ramachandran, David L Ware, Tony S Ma, John W Clark","doi":"10.1186/1742-4682-8-14","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Mathematical modeling can be employed to overcome the practical difficulty of isolating the mechanisms responsible for clinical heart failure in the setting of normal left ventricular ejection fraction (HFNEF). In a human cardiovascular respiratory system (H-CRS) model we introduce three cases of left ventricular diastolic dysfunction (LVDD): (1) impaired left ventricular active relaxation (IR-type); (2) increased passive stiffness (restrictive or R-type); and (3) the combination of both (pseudo-normal or PN-type), to produce HFNEF. The effects of increasing systolic contractility are also considered. Model results showing ensuing heart failure and mechanisms involved are reported.</p><p><strong>Methods: </strong>We employ our previously described H-CRS model with modified pulmonary compliances to better mimic normal pulmonary blood distribution. IR-type is modeled by changing the activation function of the left ventricle (LV), and R-type by increasing diastolic stiffness of the LV wall and septum. A 5th-order Cash-Karp Runge-Kutta numerical integration method solves the model differential equations.</p><p><strong>Results: </strong>IR-type and R-type decrease LV stroke volume, cardiac output, ejection fraction (EF), and mean systemic arterial pressure. Heart rate, pulmonary pressures, pulmonary volumes, and pulmonary and systemic arterial-venous O2 and CO2 differences increase. IR-type decreases, but R-type increases the mitral E/A ratio. PN-type produces the well-described, pseudo-normal mitral inflow pattern. All three types of LVDD reduce right ventricular (RV) and LV EF, but the latter remains normal or near normal. Simulations show reduced EF is partly restored by an accompanying increase in systolic stiffness, a compensatory mechanism that may lead clinicians to miss the presence of HF if they only consider LVEF and other indices of LV function. Simulations using the H-CRS model indicate that changes in RV function might well be diagnostic. This study also highlights the importance of septal mechanics in LVDD.</p><p><strong>Conclusion: </strong>The model demonstrates that abnormal LV diastolic performance alone can result in decreased LV and RV systolic performance, not previously appreciated, and contribute to the clinical syndrome of HF. Furthermore, alterations of RV diastolic performance are present and may be a hallmark of LV diastolic parameter changes that can be used for better clinical recognition of LV diastolic heart disease.</p>","PeriodicalId":51195,"journal":{"name":"Theoretical Biology and Medical Modelling","volume":" ","pages":"14"},"PeriodicalIF":0.0000,"publicationDate":"2011-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1742-4682-8-14","citationCount":"28","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Theoretical Biology and Medical Modelling","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1742-4682-8-14","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Mathematics","Score":null,"Total":0}
引用次数: 28
Abstract
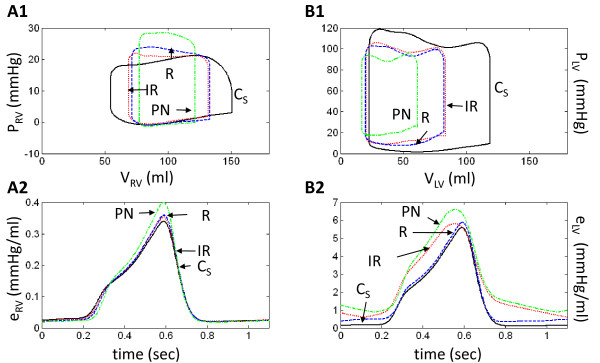
Background: Mathematical modeling can be employed to overcome the practical difficulty of isolating the mechanisms responsible for clinical heart failure in the setting of normal left ventricular ejection fraction (HFNEF). In a human cardiovascular respiratory system (H-CRS) model we introduce three cases of left ventricular diastolic dysfunction (LVDD): (1) impaired left ventricular active relaxation (IR-type); (2) increased passive stiffness (restrictive or R-type); and (3) the combination of both (pseudo-normal or PN-type), to produce HFNEF. The effects of increasing systolic contractility are also considered. Model results showing ensuing heart failure and mechanisms involved are reported.
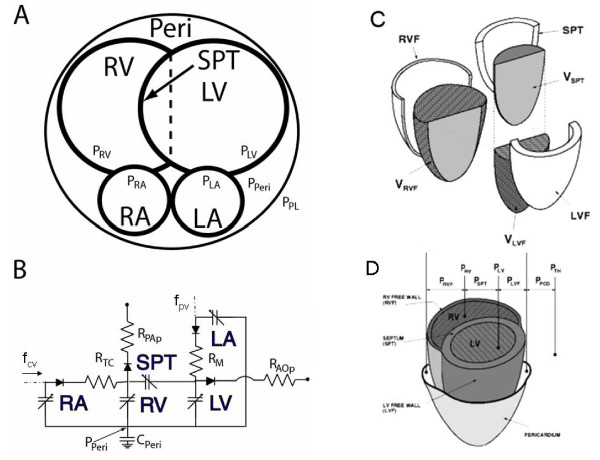
Methods: We employ our previously described H-CRS model with modified pulmonary compliances to better mimic normal pulmonary blood distribution. IR-type is modeled by changing the activation function of the left ventricle (LV), and R-type by increasing diastolic stiffness of the LV wall and septum. A 5th-order Cash-Karp Runge-Kutta numerical integration method solves the model differential equations.
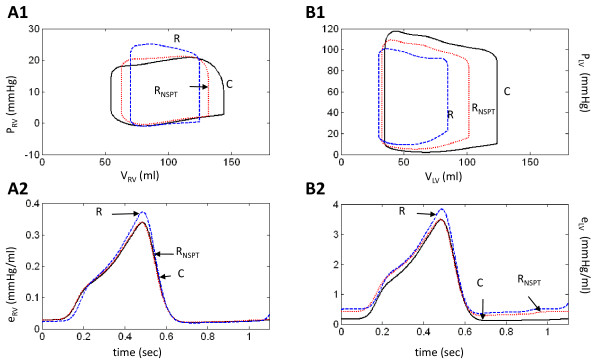
Results: IR-type and R-type decrease LV stroke volume, cardiac output, ejection fraction (EF), and mean systemic arterial pressure. Heart rate, pulmonary pressures, pulmonary volumes, and pulmonary and systemic arterial-venous O2 and CO2 differences increase. IR-type decreases, but R-type increases the mitral E/A ratio. PN-type produces the well-described, pseudo-normal mitral inflow pattern. All three types of LVDD reduce right ventricular (RV) and LV EF, but the latter remains normal or near normal. Simulations show reduced EF is partly restored by an accompanying increase in systolic stiffness, a compensatory mechanism that may lead clinicians to miss the presence of HF if they only consider LVEF and other indices of LV function. Simulations using the H-CRS model indicate that changes in RV function might well be diagnostic. This study also highlights the importance of septal mechanics in LVDD.
Conclusion: The model demonstrates that abnormal LV diastolic performance alone can result in decreased LV and RV systolic performance, not previously appreciated, and contribute to the clinical syndrome of HF. Furthermore, alterations of RV diastolic performance are present and may be a hallmark of LV diastolic parameter changes that can be used for better clinical recognition of LV diastolic heart disease.
期刊介绍:
Theoretical Biology and Medical Modelling is an open access peer-reviewed journal adopting a broad definition of "biology" and focusing on theoretical ideas and models associated with developments in biology and medicine. Mathematicians, biologists and clinicians of various specialisms, philosophers and historians of science are all contributing to the emergence of novel concepts in an age of systems biology, bioinformatics and computer modelling. This is the field in which Theoretical Biology and Medical Modelling operates. We welcome submissions that are technically sound and offering either improved understanding in biology and medicine or progress in theory or method.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


