{"title":"Biological and Environmental Factors Affecting Risk and Resilience among Syrian Refugee Children.","authors":"Arash Javanbakht, Anaïs Stenson, Nicole Nugent, Alicia Smith, David Rosenberg, Tanja Jovanovic","doi":"10.20900/jpbs.20210003","DOIUrl":null,"url":null,"abstract":"<p><p>More than 21 million people globally are refugees. More than half of these (>10 million) are children, representing a highly vulnerable population. Most children experience high levels of trauma exposure, including war trauma, as well as substantial migration- and resettlement-related stress. These exposures confer risk for mental health problems, including posttraumatic stress disorder (PTSD), but their relative contributions have not been fully explicated. These effects may be modulated by the developmental timing of trauma and stress exposure: childhood trauma and stress are broadly linked to worse health outcomes across the lifespan, but the developmental specificity of these effects remains uncertain. Refugee children typically experience the trauma leading up to displacement (e.g., civil war) which often lasts for decades, and for some, followed by resettlement. Longitudinal studies that follow children through this process can provide unique insight into how these experiences of trauma, displacement, and resettlement during development impact mechanisms of risk and resilience. They can also elucidate how environmental and physiological factors may modulate the effects of trauma and stress. The present study includes two groups of families (parents and their 7- to 17-year-old children): (1) Syrian and Iraqi refugee families who experienced war-zone trauma before resettling in the United States in ~2016, and (2) Arab immigrant families who did not experience war-zone trauma prior to resettlement in the United States in ~2016. We assessed symptoms of anxiety, depression, and PTSD in refugee and immigrant children and parents. Skin conductance responses, a measure of autonomic response, saliva samples for genetic and epigenetic analyses, and information about social and environmental context, including family structure, resources, and neighborhood quality, were also collected. Refugee participants provided data at three time points spanning ~3 years following resettlement in the United States: Wave 1, within 1 month of resettlement, Wave 2, 12-24 months post resettlement, and Wave 3 planned for 24-36 months resettlement. Immigrant participants will provide data once, within 3-5 years after immigration, matching the age of Wave 1. This comparison group enables us to compare mental health and biomarkers between refugees and immigrants. Results of these comparative analyses will provide insight into the impact of war trauma versus other types of trauma and adversity on biomarkers of child mental health outcomes. Results from the longitudinal analyses will address refugee mental health trajectories over time, and, in children, across development. Initial data from Wave 1 showed high levels of anxiety in refugee children, as well as high levels of PTSD symptoms and anxiety in their parents. Together, results from these comparative and longitudinal analyses will provide insight into multiple aspects of trauma and stress exposure in refugees and immigrants, including how the developmental timing of trauma exposure impacts biomarkers and mental health across development. Our assessment of multiple factors affecting childhood mental health following trauma exposure, including familial, neighborhood and social context following resettlement may identify modifiable targets for interventions to support well-being in refugees.</p>","PeriodicalId":73912,"journal":{"name":"Journal of psychiatry and brain science","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8009534/pdf/","citationCount":"13","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of psychiatry and brain science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20900/jpbs.20210003","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/2/24 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 13
Abstract
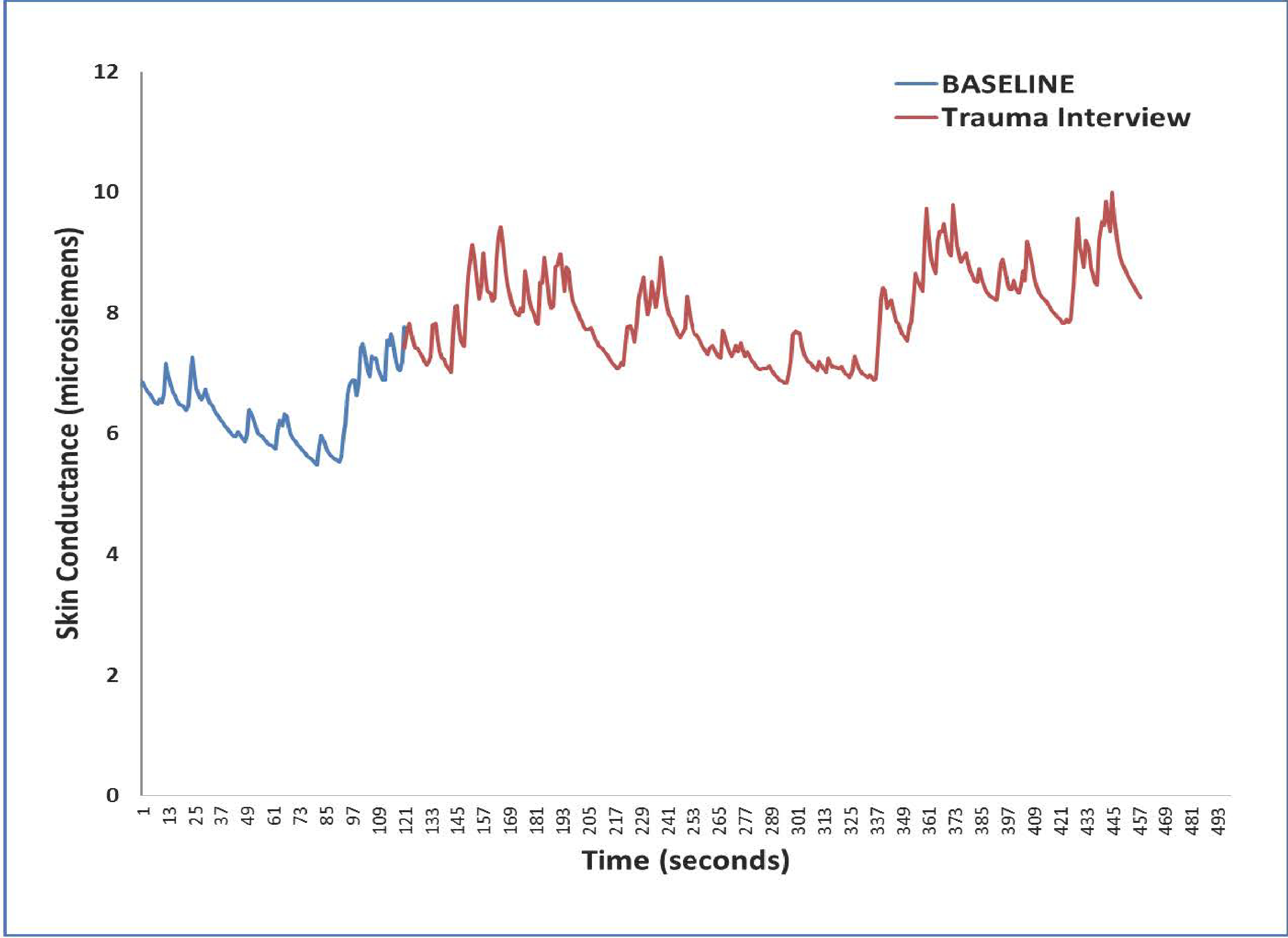
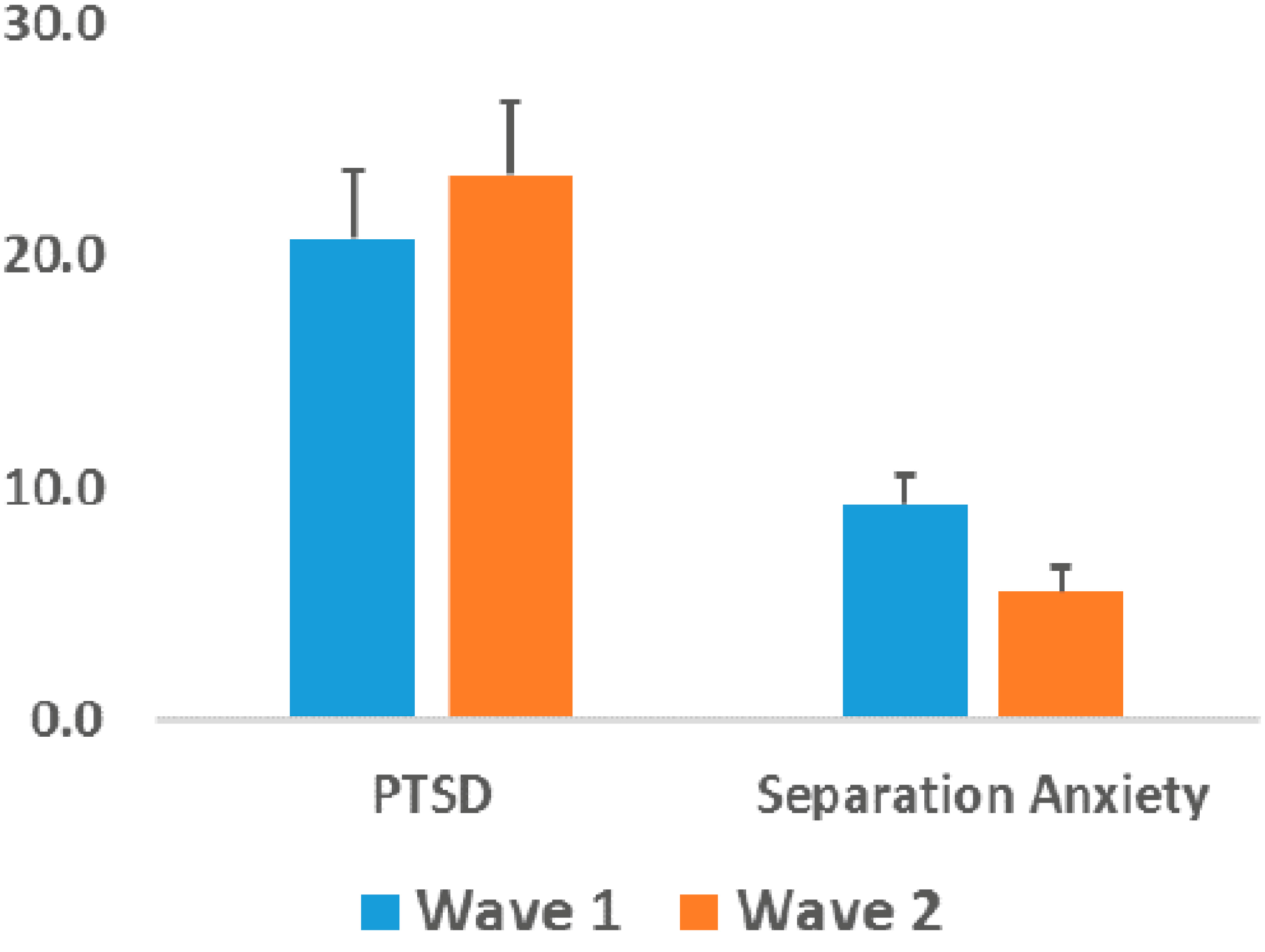
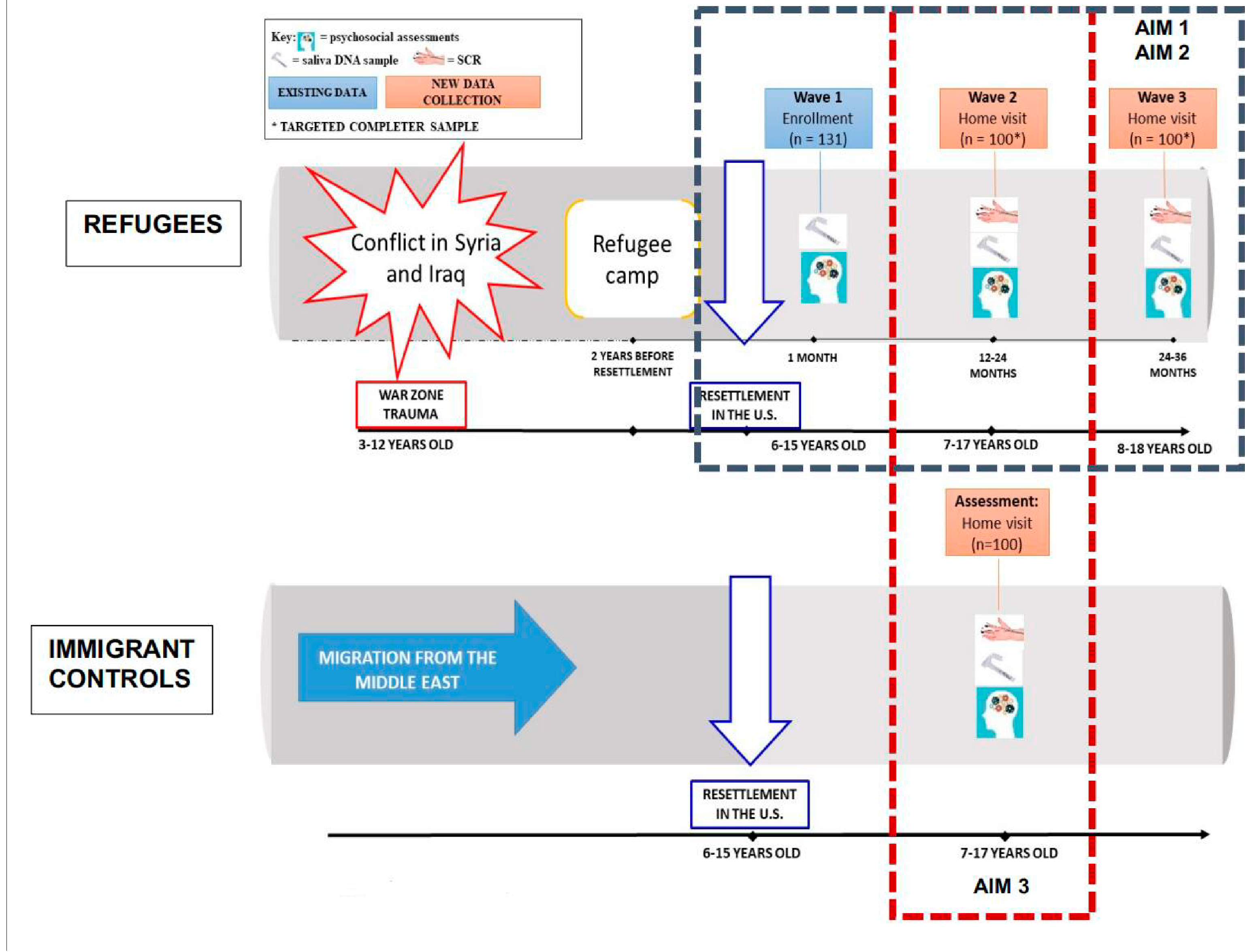
More than 21 million people globally are refugees. More than half of these (>10 million) are children, representing a highly vulnerable population. Most children experience high levels of trauma exposure, including war trauma, as well as substantial migration- and resettlement-related stress. These exposures confer risk for mental health problems, including posttraumatic stress disorder (PTSD), but their relative contributions have not been fully explicated. These effects may be modulated by the developmental timing of trauma and stress exposure: childhood trauma and stress are broadly linked to worse health outcomes across the lifespan, but the developmental specificity of these effects remains uncertain. Refugee children typically experience the trauma leading up to displacement (e.g., civil war) which often lasts for decades, and for some, followed by resettlement. Longitudinal studies that follow children through this process can provide unique insight into how these experiences of trauma, displacement, and resettlement during development impact mechanisms of risk and resilience. They can also elucidate how environmental and physiological factors may modulate the effects of trauma and stress. The present study includes two groups of families (parents and their 7- to 17-year-old children): (1) Syrian and Iraqi refugee families who experienced war-zone trauma before resettling in the United States in ~2016, and (2) Arab immigrant families who did not experience war-zone trauma prior to resettlement in the United States in ~2016. We assessed symptoms of anxiety, depression, and PTSD in refugee and immigrant children and parents. Skin conductance responses, a measure of autonomic response, saliva samples for genetic and epigenetic analyses, and information about social and environmental context, including family structure, resources, and neighborhood quality, were also collected. Refugee participants provided data at three time points spanning ~3 years following resettlement in the United States: Wave 1, within 1 month of resettlement, Wave 2, 12-24 months post resettlement, and Wave 3 planned for 24-36 months resettlement. Immigrant participants will provide data once, within 3-5 years after immigration, matching the age of Wave 1. This comparison group enables us to compare mental health and biomarkers between refugees and immigrants. Results of these comparative analyses will provide insight into the impact of war trauma versus other types of trauma and adversity on biomarkers of child mental health outcomes. Results from the longitudinal analyses will address refugee mental health trajectories over time, and, in children, across development. Initial data from Wave 1 showed high levels of anxiety in refugee children, as well as high levels of PTSD symptoms and anxiety in their parents. Together, results from these comparative and longitudinal analyses will provide insight into multiple aspects of trauma and stress exposure in refugees and immigrants, including how the developmental timing of trauma exposure impacts biomarkers and mental health across development. Our assessment of multiple factors affecting childhood mental health following trauma exposure, including familial, neighborhood and social context following resettlement may identify modifiable targets for interventions to support well-being in refugees.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


