{"title":"Sinking Skin Flap Syndrome following Posttraumatic Hydrocephalus.","authors":"Ashish Chugh, Prashant Punia, Sarang Gotecha","doi":"10.1155/2021/6682310","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Complications following craniotomy are not uncommon and Sinking Skin Flap Syndrome (SSFS) constitutes a rare entity that may present after a large Decompressive Craniectomy. Although the entity is widely reported, the literature mostly consists of case reports. Authors present a case series of three patients with review of literature highlighting the various factors which can prove therapeutic and can help in avoidance of complications.</p><p><strong>Materials and methods: </strong>The study was conducted over a period of 3 years, from 2016 to 2019, and included 212 patients who underwent unilateral Decompressive Craniectomy (DC) for trauma in our institute. All 212 patients underwent a similar DC following a strict institutional protocol and the craniectomies were performed by the same surgical team. At total of 160 patients survived and elective cranioplasty was planned at a 3-month interval. Out of a total of 160 patients who survived, 38 developed hydrocephalus, 3 patients presented with hydrocephalus acutely and had to be shunted before cranioplasty and underwent ventriculoperitoneal (VP) shunting on the opposite side of craniectomy. All 3 of these patients developed SSFS and were the focus of this case series wherein review of literature was done with emphasis being laid on the salient features towards management of SSFS in such precranioplasty shunted patients. These 3 patients were treated via rehydration using normal saline (NS) till the Central Venous Pressure (CVP) equaled 8-10 cm of water, nursing in Trendelenburg position and shunt occlusion using silk 3-0 round bodied suture tied over a \"C\"-loop of VP shunt tube over clavicle. This was followed by cranioplasty within 2 days of presentation using a flattened, nonconvex artificial Polymethyl Methacrylate (PMMA) bone flap with central hitch suture taken across the bone flap and release of shunt tie in immediate postoperative period. The PMMA bone flap was made intraoperatively after measuring the defect size accurately after exposure of defect. 3D printing option was not availed by any patient considering the high cost and patients' poor socioeconomic status.</p><p><strong>Results: </strong>Out of a total of 212 patients, thirty-eight patients (19%) developed posttraumatic hydrocephalus and out of 38, three presented with SSFS over the course of time. Two patients presented with hemiparesis of the side opposite to sunken flap while 1 other patient was brought by relatives in stuporous state. All 3 were subjected to VP shunt tie, rehydration, and cranioplasty using flattened artificial bone flap and showed gradual recovery in postoperative period without any complications.</p><p><strong>Conclusion: </strong>Various factors like nursing in Trendelenburg position, adequate rehydration, early cranioplasty after resolution of oedema, preoperative tying of VP shunt and its subsequent release in immediate postoperative period, use of flattened PMMA bone flaps, placement of a central dural hitch suture across the bone, and a preoperative central burr hole in the bone flap may accelerate healing and, in most cases, reversal of sensory-motor deficits along with reduction in complication rates.</p>","PeriodicalId":9615,"journal":{"name":"Case Reports in Neurological Medicine","volume":" ","pages":"6682310"},"PeriodicalIF":0.9000,"publicationDate":"2021-02-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7886569/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Neurological Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/6682310","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 2
Abstract
Introduction: Complications following craniotomy are not uncommon and Sinking Skin Flap Syndrome (SSFS) constitutes a rare entity that may present after a large Decompressive Craniectomy. Although the entity is widely reported, the literature mostly consists of case reports. Authors present a case series of three patients with review of literature highlighting the various factors which can prove therapeutic and can help in avoidance of complications.
Materials and methods: The study was conducted over a period of 3 years, from 2016 to 2019, and included 212 patients who underwent unilateral Decompressive Craniectomy (DC) for trauma in our institute. All 212 patients underwent a similar DC following a strict institutional protocol and the craniectomies were performed by the same surgical team. At total of 160 patients survived and elective cranioplasty was planned at a 3-month interval. Out of a total of 160 patients who survived, 38 developed hydrocephalus, 3 patients presented with hydrocephalus acutely and had to be shunted before cranioplasty and underwent ventriculoperitoneal (VP) shunting on the opposite side of craniectomy. All 3 of these patients developed SSFS and were the focus of this case series wherein review of literature was done with emphasis being laid on the salient features towards management of SSFS in such precranioplasty shunted patients. These 3 patients were treated via rehydration using normal saline (NS) till the Central Venous Pressure (CVP) equaled 8-10 cm of water, nursing in Trendelenburg position and shunt occlusion using silk 3-0 round bodied suture tied over a "C"-loop of VP shunt tube over clavicle. This was followed by cranioplasty within 2 days of presentation using a flattened, nonconvex artificial Polymethyl Methacrylate (PMMA) bone flap with central hitch suture taken across the bone flap and release of shunt tie in immediate postoperative period. The PMMA bone flap was made intraoperatively after measuring the defect size accurately after exposure of defect. 3D printing option was not availed by any patient considering the high cost and patients' poor socioeconomic status.
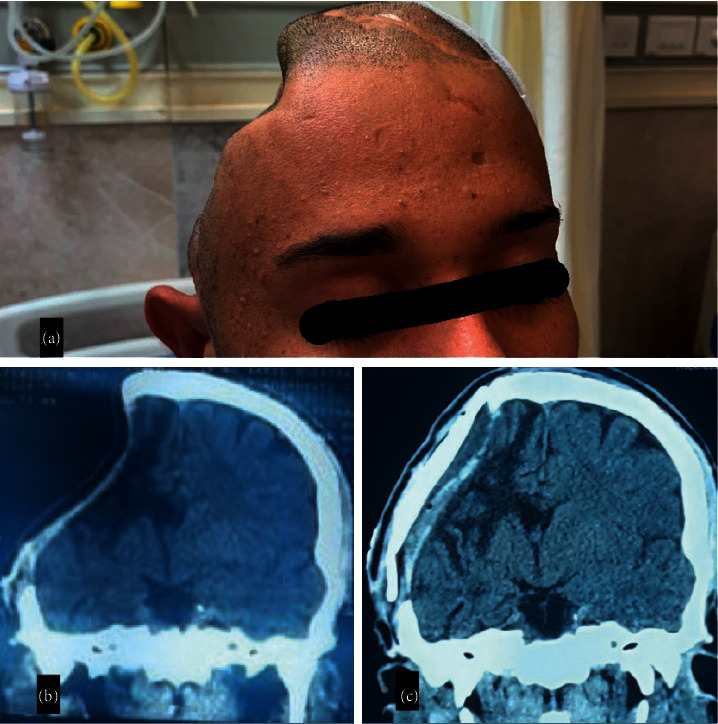
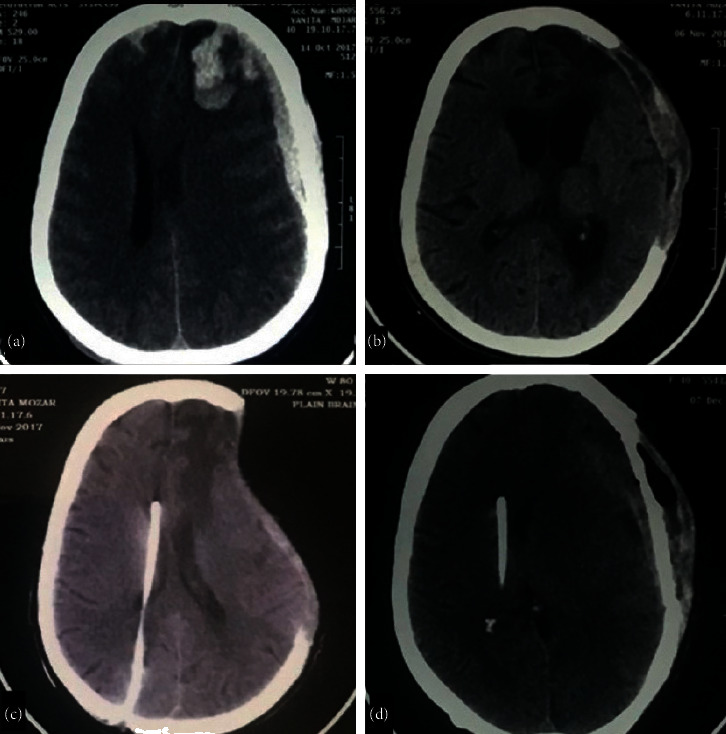
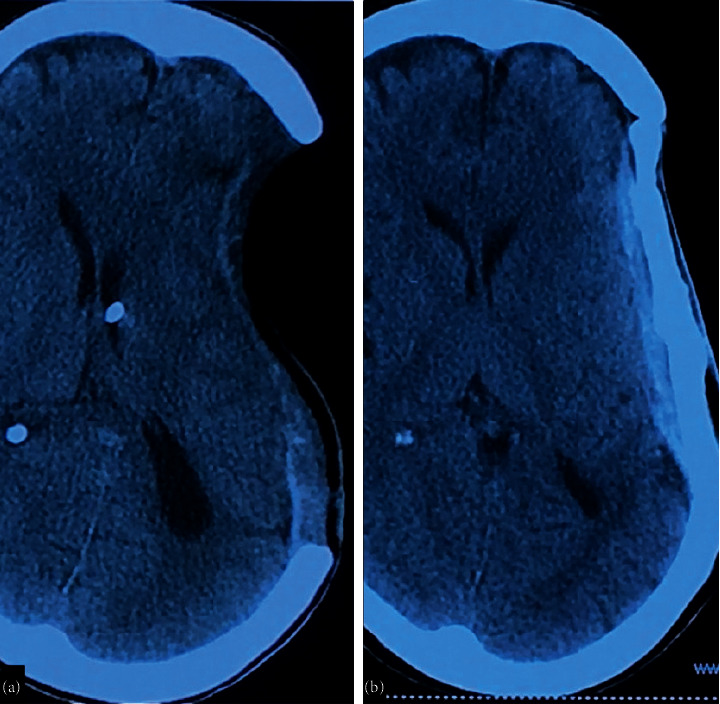
Results: Out of a total of 212 patients, thirty-eight patients (19%) developed posttraumatic hydrocephalus and out of 38, three presented with SSFS over the course of time. Two patients presented with hemiparesis of the side opposite to sunken flap while 1 other patient was brought by relatives in stuporous state. All 3 were subjected to VP shunt tie, rehydration, and cranioplasty using flattened artificial bone flap and showed gradual recovery in postoperative period without any complications.
Conclusion: Various factors like nursing in Trendelenburg position, adequate rehydration, early cranioplasty after resolution of oedema, preoperative tying of VP shunt and its subsequent release in immediate postoperative period, use of flattened PMMA bone flaps, placement of a central dural hitch suture across the bone, and a preoperative central burr hole in the bone flap may accelerate healing and, in most cases, reversal of sensory-motor deficits along with reduction in complication rates.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


