{"title":"Cutaneous Coinfection of Cytomegalovirus and <i>Mycobacterium chelonae</i> Accelerated by Immunosuppression.","authors":"Yutaka Tsutsumi, Kentaro Odani, Yasuhito Kaneko, Hideo Hashizume, Mitsuhiro Tachibana","doi":"10.1155/2021/8819560","DOIUrl":null,"url":null,"abstract":"<p><p>A mildly diabetic 58-year-old male had traumatic ulceration on the left popliteal fossa, and the lesion progressed to a painful 6 cm deep ulcer. After surgical debridement and skin grafting, ulceration recurred. Pyoderma gangrenosum was clinically diagnosed after the first biopsy, indicating a noninfective ulcer. Immunosuppressive therapy (prednisolone and cyclosporine A) induced complete epithelialization in three months. Four months later, subcutaneous nonulcerated nodules appeared on the anterior area of the left lower leg. Subcutaneous induration progressed and ulceration recurred, so that immunosuppressive therapy continued for one year. Cytomegalovirus (CMV) viremia was detected, and the second biopsy demonstrated CMV inclusions of endothelial and perivascular cells in fibrosing septolobular panniculitis. Cyclosporine A was cancelled, prednisolone was tapered, and ganciclovir started. Viremia soon disappeared, but the lesion progressed to large induration with multiple ulcers measuring up to 3 cm. The third biopsy disclosed infection of Gram-positive mycobacteria, accompanying fat droplet-centered suppurative granulomas without CMV infection. Microbial culture identified <i>Mycobacterium chelonae</i>. Clarithromycin with thermotherapy was effective. A review of the second biopsy confirmed coinfection of CMV and Gram-positive mycobacteria. Immunostaining using a panel of anti-bacterial antibodies visualized the mycobacteria in the lesion. Positive findings were obtained with antibodies to Bacillus Calmette-Guérin, <i>Bacillus cereus</i>, MPT64 (<i>Mycobacterium tuberculosis</i>-specific 24 kDa secretory antigen), LAM (<i>Mycobacterium tuberculosis</i>-related lipoarabinomannan), and PAB (<i>Propionibacterium acnes</i>-specific lipoteichoic acid).</p>","PeriodicalId":45638,"journal":{"name":"Case Reports in Pathology","volume":"2021 ","pages":"8819560"},"PeriodicalIF":0.7000,"publicationDate":"2021-01-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7867456/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Pathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/8819560","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"PATHOLOGY","Score":null,"Total":0}
引用次数: 2
Abstract
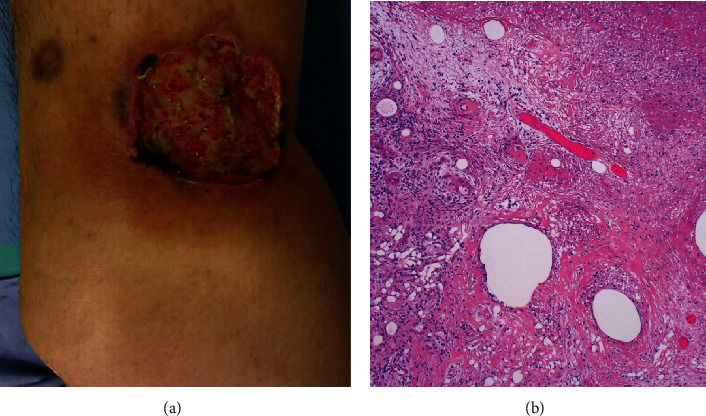
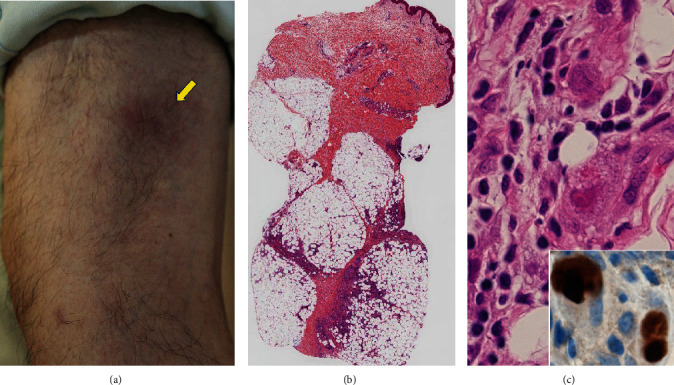
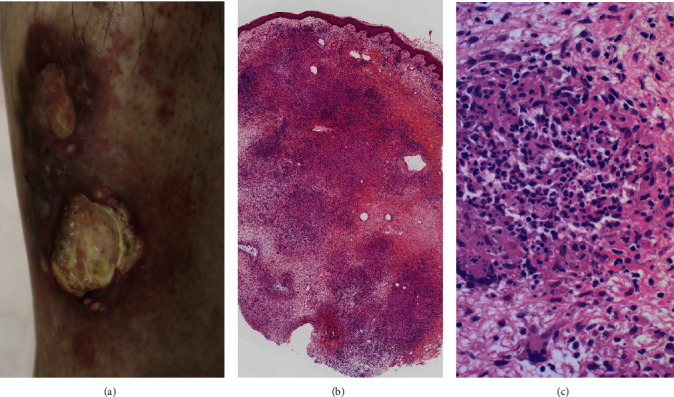
A mildly diabetic 58-year-old male had traumatic ulceration on the left popliteal fossa, and the lesion progressed to a painful 6 cm deep ulcer. After surgical debridement and skin grafting, ulceration recurred. Pyoderma gangrenosum was clinically diagnosed after the first biopsy, indicating a noninfective ulcer. Immunosuppressive therapy (prednisolone and cyclosporine A) induced complete epithelialization in three months. Four months later, subcutaneous nonulcerated nodules appeared on the anterior area of the left lower leg. Subcutaneous induration progressed and ulceration recurred, so that immunosuppressive therapy continued for one year. Cytomegalovirus (CMV) viremia was detected, and the second biopsy demonstrated CMV inclusions of endothelial and perivascular cells in fibrosing septolobular panniculitis. Cyclosporine A was cancelled, prednisolone was tapered, and ganciclovir started. Viremia soon disappeared, but the lesion progressed to large induration with multiple ulcers measuring up to 3 cm. The third biopsy disclosed infection of Gram-positive mycobacteria, accompanying fat droplet-centered suppurative granulomas without CMV infection. Microbial culture identified Mycobacterium chelonae. Clarithromycin with thermotherapy was effective. A review of the second biopsy confirmed coinfection of CMV and Gram-positive mycobacteria. Immunostaining using a panel of anti-bacterial antibodies visualized the mycobacteria in the lesion. Positive findings were obtained with antibodies to Bacillus Calmette-Guérin, Bacillus cereus, MPT64 (Mycobacterium tuberculosis-specific 24 kDa secretory antigen), LAM (Mycobacterium tuberculosis-related lipoarabinomannan), and PAB (Propionibacterium acnes-specific lipoteichoic acid).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


