{"title":"Pharmacokinetics and Toxicities of Oral Docetaxel Formulations Co-Administered with Ritonavir in Phase I Trials.","authors":"Marit Vermunt, Serena Marchetti, Jos Beijnen","doi":"10.2147/CPAA.S292746","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Docetaxel is widely used as intravenous (IV) chemotherapy. Oral docetaxel is co-administered with the cytochrome P450 3A4 and P-glycoprotein inhibitor ritonavir to increase oral bioavailability. This research explores the relationship between the pharmacokinetics (PK) and toxicity of this novel oral chemotherapy.</p><p><strong>Methods: </strong>The patients in two phase I trials were treated with different oral docetaxel formulations in combination with ritonavir in different dose levels, ranging from 20 to 80 mg docetaxel with 100 to 200 mg ritonavir a day. The patients were categorized based on the absence or occurrence of severe treatment-related toxicity (grade ≥3 or any grade leading to treatment alterations). The docetaxel area under the plasma concentration-time curve (AUC) and maximum plasma concentration (C<sub>max</sub>) were associated with toxicity.</p><p><strong>Results: </strong>Thirty-four out of 138 patients experienced severe toxicity, most frequently observed as mucositis, fatigue, diarrhea, nausea and vomiting. The severe toxicity group had a significantly higher docetaxel AUC (2231 ± 1405 vs 1011 ± 830 ng/mL*h, p<0.0001) and C<sub>max</sub> (218 ± 178 vs 119 ± 77 ng/mL, p<0.0001) as compared to the patients without severe toxicity. When extrapolated from IV PK data, the patients without severe toxicity had a similar cumulative docetaxel AUC as with standard 3-weekly IV docetaxel, while the C<sub>max</sub> was up to 10-fold lower with oral docetaxel and ritonavir.</p><p><strong>Conclusion: </strong>Severe toxicity was observed in 25% of the patients treated with oral docetaxel and ritonavir. This toxicity seems related to the PK, as the docetaxel AUC<sub>0-inf</sub> and C<sub>max</sub> were up to twofold higher in the severe toxicity group as compared to the non-severe toxicity group. Future randomized trials will provide a further evaluation of the toxicity and efficacy of the new weekly oral docetaxel and ritonavir regimen in comparison to standard IV docetaxel.</p>","PeriodicalId":10406,"journal":{"name":"Clinical Pharmacology : Advances and Applications","volume":" ","pages":"21-32"},"PeriodicalIF":2.5000,"publicationDate":"2021-01-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e7/d2/cpaa-13-21.PMC7850405.pdf","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacology : Advances and Applications","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CPAA.S292746","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 6
Abstract
Introduction: Docetaxel is widely used as intravenous (IV) chemotherapy. Oral docetaxel is co-administered with the cytochrome P450 3A4 and P-glycoprotein inhibitor ritonavir to increase oral bioavailability. This research explores the relationship between the pharmacokinetics (PK) and toxicity of this novel oral chemotherapy.
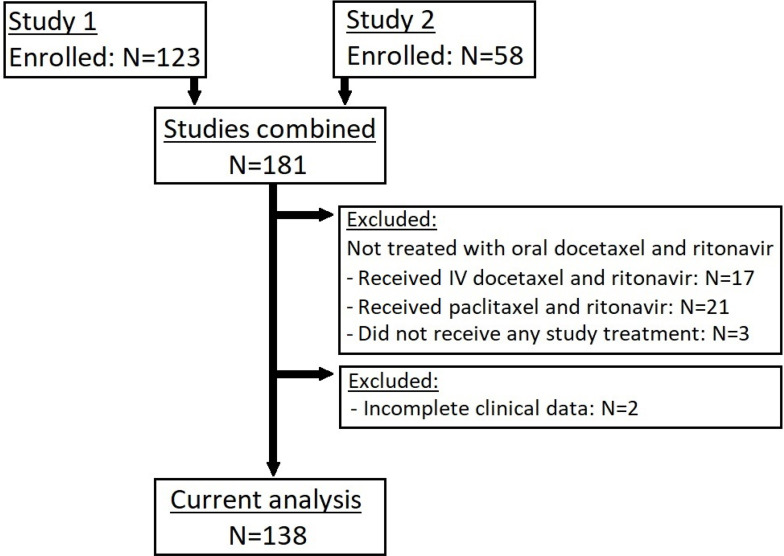
Methods: The patients in two phase I trials were treated with different oral docetaxel formulations in combination with ritonavir in different dose levels, ranging from 20 to 80 mg docetaxel with 100 to 200 mg ritonavir a day. The patients were categorized based on the absence or occurrence of severe treatment-related toxicity (grade ≥3 or any grade leading to treatment alterations). The docetaxel area under the plasma concentration-time curve (AUC) and maximum plasma concentration (Cmax) were associated with toxicity.
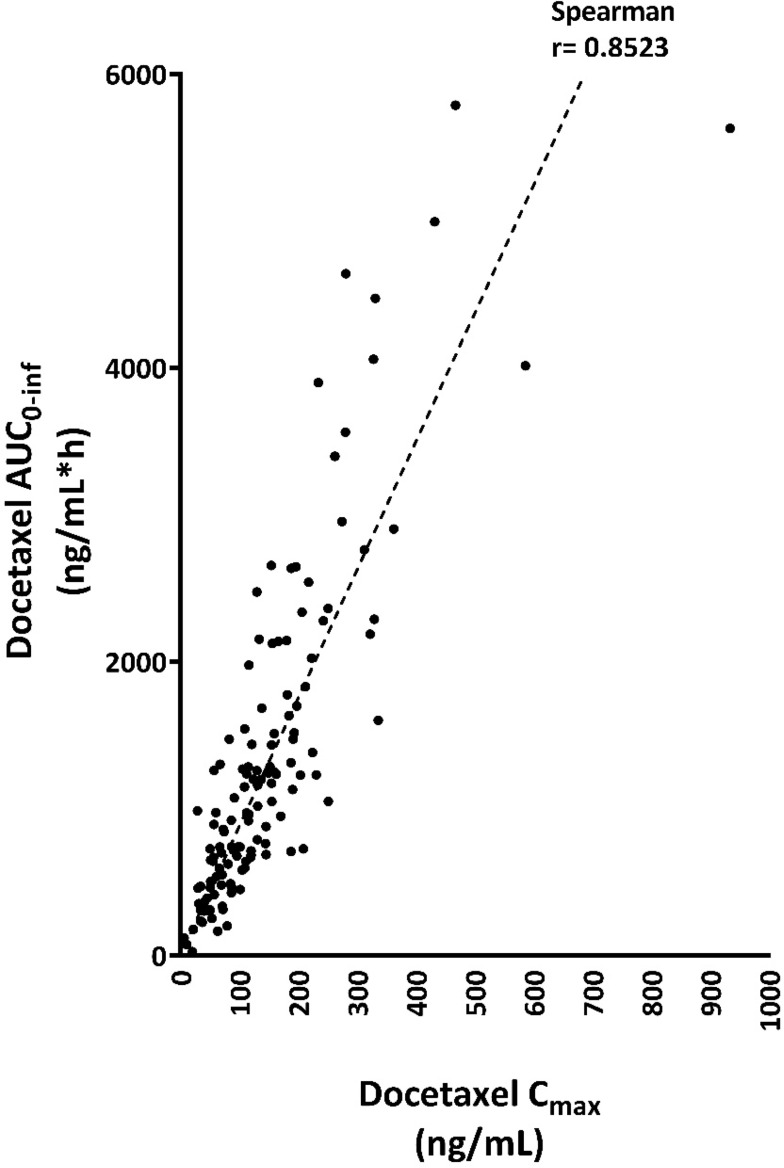
Results: Thirty-four out of 138 patients experienced severe toxicity, most frequently observed as mucositis, fatigue, diarrhea, nausea and vomiting. The severe toxicity group had a significantly higher docetaxel AUC (2231 ± 1405 vs 1011 ± 830 ng/mL*h, p<0.0001) and Cmax (218 ± 178 vs 119 ± 77 ng/mL, p<0.0001) as compared to the patients without severe toxicity. When extrapolated from IV PK data, the patients without severe toxicity had a similar cumulative docetaxel AUC as with standard 3-weekly IV docetaxel, while the Cmax was up to 10-fold lower with oral docetaxel and ritonavir.
Conclusion: Severe toxicity was observed in 25% of the patients treated with oral docetaxel and ritonavir. This toxicity seems related to the PK, as the docetaxel AUC0-inf and Cmax were up to twofold higher in the severe toxicity group as compared to the non-severe toxicity group. Future randomized trials will provide a further evaluation of the toxicity and efficacy of the new weekly oral docetaxel and ritonavir regimen in comparison to standard IV docetaxel.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


