The Impact of Medication Reviews Conducted in Primary Care on Hospital Admissions and Mortality: An Observational Follow-Up of a Randomized Controlled Trial.
{"title":"The Impact of Medication Reviews Conducted in Primary Care on Hospital Admissions and Mortality: An Observational Follow-Up of a Randomized Controlled Trial.","authors":"Veronica Milos Nymberg, Cecilia Lenander, Beata Borgström Bolmsjö","doi":"10.2147/DHPS.S283708","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Drug-related problems among the elderly population are common and increasing. Multi-professional medication reviews (MR) have arisen as a method to optimize drug therapy for frail elderly patients. Research has not yet been able to show conclusive evidence of the effect of MRs on mortality or hospital admissions.</p><p><strong>Aim: </strong>The aim of this study was to assess the impact of MRs' on hospital admissions and mortality after six and 12 months in a frail population of 369 patients in primary care in a cohort from a randomized controlled study.</p><p><strong>Methods: </strong>Patients were blindly randomized to an intervention group (receiving MRs) and a control group (receiving usual care). Descriptive data on mortality and hospital admissions at six and 12 months were collected. Survival analysis was performed for time to death and time to the first hospital admission within 12 months.</p><p><strong>Results: </strong>An observational follow-up was performed in a cohort of 369 patients, previously randomized to an intervention group (182) and a control group (187). Most of the patients (75%) were females and lived in nursing homes. At six months, 50 patients of the baseline population (27%) in the control group had been admitted to hospital at least once, compared to 40 patients (21%) in the intervention group. At 12 months, the percentage had increased to 70 (37%) in the control group compared to 53 (29%) in the intervention group. Compared to usual care, we found that MRs reduced the risk of hospital admissions within 12 months by 42% (HR = 0.58, 95% CI 0.37-0.92, p=0.021), but found no difference in mortality (HR = 1.12, 95% CI 0.78-1.61, p=0.551) between the groups.</p><p><strong>Conclusion: </strong>We suggest that MRs should be recommended in the care of frail elderly patients with expected benefits on delayed hospital admissions. The study is registered at ClinicalTrials.gov, registration number NCT04040855, Unique Protocol ID 2018/8.</p>","PeriodicalId":11377,"journal":{"name":"Drug, Healthcare and Patient Safety","volume":"13 ","pages":"1-9"},"PeriodicalIF":3.4000,"publicationDate":"2021-01-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/83/65/dhps-13-1.PMC7850439.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug, Healthcare and Patient Safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/DHPS.S283708","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 2
Abstract
Background: Drug-related problems among the elderly population are common and increasing. Multi-professional medication reviews (MR) have arisen as a method to optimize drug therapy for frail elderly patients. Research has not yet been able to show conclusive evidence of the effect of MRs on mortality or hospital admissions.
Aim: The aim of this study was to assess the impact of MRs' on hospital admissions and mortality after six and 12 months in a frail population of 369 patients in primary care in a cohort from a randomized controlled study.
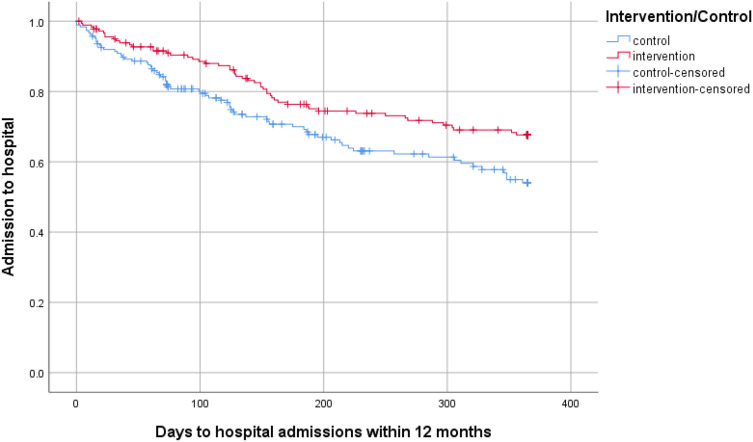
Methods: Patients were blindly randomized to an intervention group (receiving MRs) and a control group (receiving usual care). Descriptive data on mortality and hospital admissions at six and 12 months were collected. Survival analysis was performed for time to death and time to the first hospital admission within 12 months.
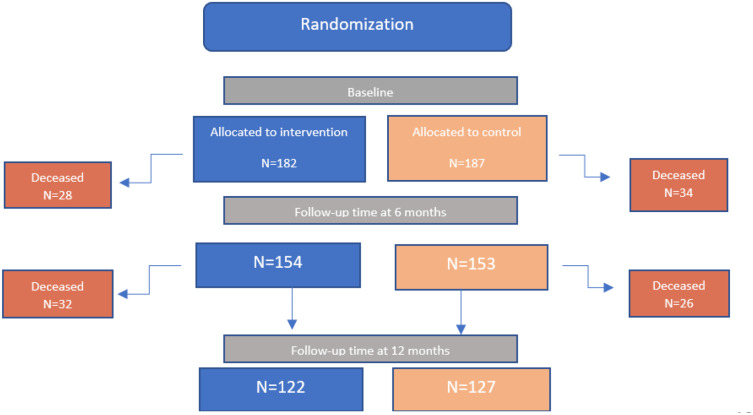
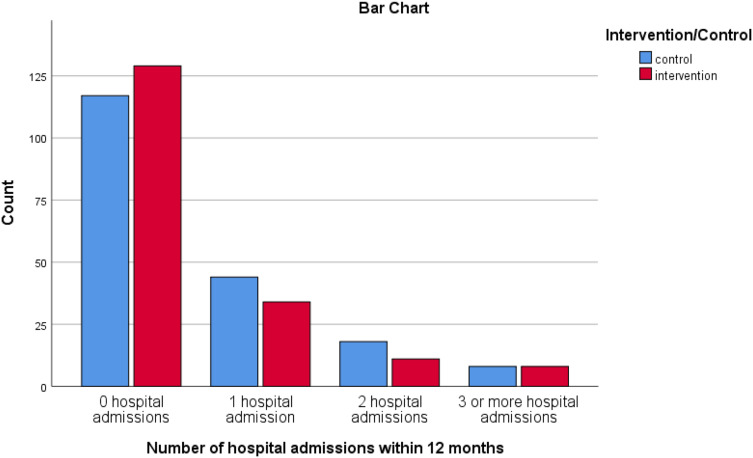
Results: An observational follow-up was performed in a cohort of 369 patients, previously randomized to an intervention group (182) and a control group (187). Most of the patients (75%) were females and lived in nursing homes. At six months, 50 patients of the baseline population (27%) in the control group had been admitted to hospital at least once, compared to 40 patients (21%) in the intervention group. At 12 months, the percentage had increased to 70 (37%) in the control group compared to 53 (29%) in the intervention group. Compared to usual care, we found that MRs reduced the risk of hospital admissions within 12 months by 42% (HR = 0.58, 95% CI 0.37-0.92, p=0.021), but found no difference in mortality (HR = 1.12, 95% CI 0.78-1.61, p=0.551) between the groups.
Conclusion: We suggest that MRs should be recommended in the care of frail elderly patients with expected benefits on delayed hospital admissions. The study is registered at ClinicalTrials.gov, registration number NCT04040855, Unique Protocol ID 2018/8.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


