{"title":"Multimodal Brain Monitoring-Guided Anesthesia Management Improves Functional Connectivity, Enhances Recovery and Attenuates Postoperative Pain in Elderly Surgical Patients.","authors":"Shuyi Yang, Shuai Feng, Hao Wu, Chonglin Zhong, Shubin Zhan, Chunxiu Wang, Zan Chen, Yaxian Huang, Guanxu Zhao, Yue Zhang, Tianlong Wang, Wei Xiao","doi":"10.2147/CIA.S551727","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Perioperative neurocognitive disorder (PND) is common in elderly surgical patients and severely affects postoperative recovery. However, effective prevention is still lacking. Potential perioperative cerebral stressors (including inappropriate sedative/analgesic depth and imbalanced cerebral oxygen supply/demand) may be important contributing factors. We developed an anesthesia management protocol based on multimodal brain monitoring to achieve standardized, individualized, and real-time regulation of sedative/analgesic depth and cerebral oxygen saturation and investigated whether it could reduce the incidence of PND and its underlying mechanisms.</p><p><strong>Patients and methods: </strong>Patients (aged ≥65 years) were randomized into Groups C (n=88) and E (n=93). Patients in Group E received multimodal brain monitoring-guided anesthesia management, and those in Group C received BIS-guided anesthesia management. The Montreal Cognitive Assessment (MoCA) was performed both before and seven days after surgery. The postoperative pain scores were recorded. Resting-state functional MRI data were analyzed to examine functional connectivity (FC).</p><p><strong>Results: </strong>Group E demonstrated a numerically lower incidence of PND (15.50% vs 21.59% in Group C), but this difference was not statistically significant. Patients in Group E had increased FC within the right pulvinar, right sub-gyral region, and right inferior parietal lobule (<i>P</i> < 0.05). Significantly lower pain scores were observed in Group E at rest (1h: <i>P</i>=0.04; 24h: <i>P</i>=0.04) and during movement (1h: <i>P</i>=0.03).</p><p><strong>Conclusion: </strong>These results suggest that multimodal brain monitoring-guided anesthesia management may protect neurocognition by enhancing FC within cognition-associated brain regions and attenuating postoperative acute pain. And multimodal brain monitoring-guided anesthesia management may confer a clinically relevant reduction in PND incidence compared to BIS-guided management in elderly surgical patients.</p>","PeriodicalId":48841,"journal":{"name":"Clinical Interventions in Aging","volume":"20 ","pages":"1757-1771"},"PeriodicalIF":3.7000,"publicationDate":"2025-10-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12535745/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Interventions in Aging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/CIA.S551727","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Perioperative neurocognitive disorder (PND) is common in elderly surgical patients and severely affects postoperative recovery. However, effective prevention is still lacking. Potential perioperative cerebral stressors (including inappropriate sedative/analgesic depth and imbalanced cerebral oxygen supply/demand) may be important contributing factors. We developed an anesthesia management protocol based on multimodal brain monitoring to achieve standardized, individualized, and real-time regulation of sedative/analgesic depth and cerebral oxygen saturation and investigated whether it could reduce the incidence of PND and its underlying mechanisms.
Patients and methods: Patients (aged ≥65 years) were randomized into Groups C (n=88) and E (n=93). Patients in Group E received multimodal brain monitoring-guided anesthesia management, and those in Group C received BIS-guided anesthesia management. The Montreal Cognitive Assessment (MoCA) was performed both before and seven days after surgery. The postoperative pain scores were recorded. Resting-state functional MRI data were analyzed to examine functional connectivity (FC).
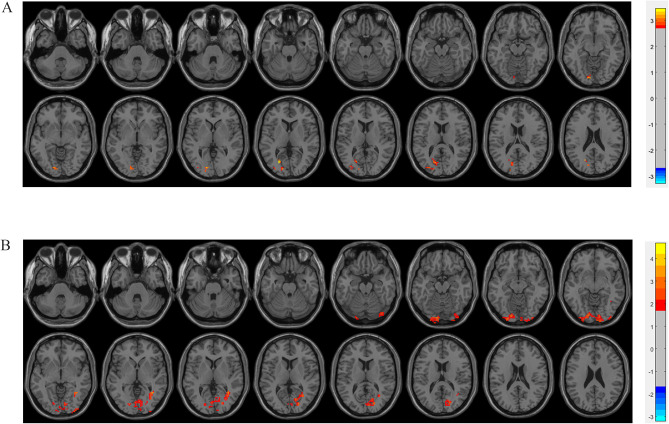
Results: Group E demonstrated a numerically lower incidence of PND (15.50% vs 21.59% in Group C), but this difference was not statistically significant. Patients in Group E had increased FC within the right pulvinar, right sub-gyral region, and right inferior parietal lobule (P < 0.05). Significantly lower pain scores were observed in Group E at rest (1h: P=0.04; 24h: P=0.04) and during movement (1h: P=0.03).
Conclusion: These results suggest that multimodal brain monitoring-guided anesthesia management may protect neurocognition by enhancing FC within cognition-associated brain regions and attenuating postoperative acute pain. And multimodal brain monitoring-guided anesthesia management may confer a clinically relevant reduction in PND incidence compared to BIS-guided management in elderly surgical patients.
期刊介绍:
Clinical Interventions in Aging, is an online, peer reviewed, open access journal focusing on concise rapid reporting of original research and reviews in aging. Special attention will be given to papers reporting on actual or potential clinical applications leading to improved prevention or treatment of disease or a greater understanding of pathological processes that result from maladaptive changes in the body associated with aging. This journal is directed at a wide array of scientists, engineers, pharmacists, pharmacologists and clinical specialists wishing to maintain an up to date knowledge of this exciting and emerging field.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


