Transarterial Embolization for Refractory Non-Cervical-Origin Interscapular Pain Following Ultrasound-Guided Injection: A Retrospective Feasibility Study.
{"title":"Transarterial Embolization for Refractory Non-Cervical-Origin Interscapular Pain Following Ultrasound-Guided Injection: A Retrospective Feasibility Study.","authors":"Yu-Han Huang, Chia-Wei Chang, Jui-Yuan Chen, Chia-Shiang Lin, Chun-Wei Lin, Ping-Sheng Lu, Neng-Yu Chiu, Keng-Wei Liang","doi":"10.3390/diagnostics15192496","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objective</b>: Chronic non-cervical-origin interscapular pain remains challenging to treat when refractory to conservative management and ultrasound-guided injections. This retrospective feasibility study aimed to assess the feasibility, procedural practicality, safety, and preliminary clinical outcomes of transarterial embolization (TAE) as a salvage therapy in this patient population. <b>Methods</b>: This single-center retrospective study included 20 patients with chronic interscapular pain (Numeric Rating Scale [NRS] score ≥5 for >3 months) who initially underwent ultrasound-guided injection therapy. Patients who experienced inadequate pain relief after 3 months (<i>n</i> = 10) proceeded to TAE, while the remaining 10 patients with sufficient relief formed the comparison group. TAE primarily targeted the transverse cervical artery using imipenem/cilastatin sodium as the embolic agent. Pain outcomes were assessed using NRS scores at 1, 3, and 6 months post-procedure. The primary outcome was pain reduction (≥50% decrease in NRS score), with secondary outcomes including technical success, medication use, and safety assessment. <b>Results</b>: The mean baseline NRS score for all patients was 6.5 ± 1.4, which decreased to 3.4 ± 2.0 at 1 month and 3.9 ± 2.5 at 3 months post-injection (<i>p</i> < 0.001). In the TAE group, the NRS score decreased from 7.4 ± 1.4 to 5.1 ± 1.1 at 1 month and 6.0 ± 1.4 at 3 months, indicating inadequate pain relief. In contrast, the injection-only group showed significant improvement, with NRS scores decreasing from 5.6 ± 0.5 to 1.6 ± 0.5 at 1 month and 1.7 ± 0.7 at 3 months (<i>p</i> < 0.001). The reduction in NRS scores was significantly less in the TAE group compared with the injection-only group (-2.2 vs. -4.0 and -28.7% vs. -71.4% at 1 month; -1.4 vs. -3.9 and -18.2% vs. -69.7% at 3 months; all <i>p</i> ≤ 0.001). Following TAE, the mean NRS score further decreased to 2.1 ± 0.7, 2.0 ± 1.1, and 1.9 ± 1.2 at 1, 3, and 6 months, respectively (<i>p</i> < 0.001), with clinical success rates of 90%, 100%, and 90% at these respective time points. At the final follow-up, the percentage of NRS score reduction was comparable between the TAE and injection-only groups (-74.8% vs. -69.7%, <i>p</i> = 0.397). No severe or life-threatening adverse events were observed; only self-limited adverse events were reported. <b>Conclusions</b>: In this retrospective feasibility study, TAE appeared safe and effective as a salvage therapy for patients with refractory non-cervical-origin interscapular pain unresponsive to injection therapy. Further prospective, randomized studies are needed to validate these findings, refine patient selection criteria, and optimize treatment outcomes.</p>","PeriodicalId":11225,"journal":{"name":"Diagnostics","volume":"15 19","pages":""},"PeriodicalIF":3.3000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12523267/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diagnostics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/diagnostics15192496","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
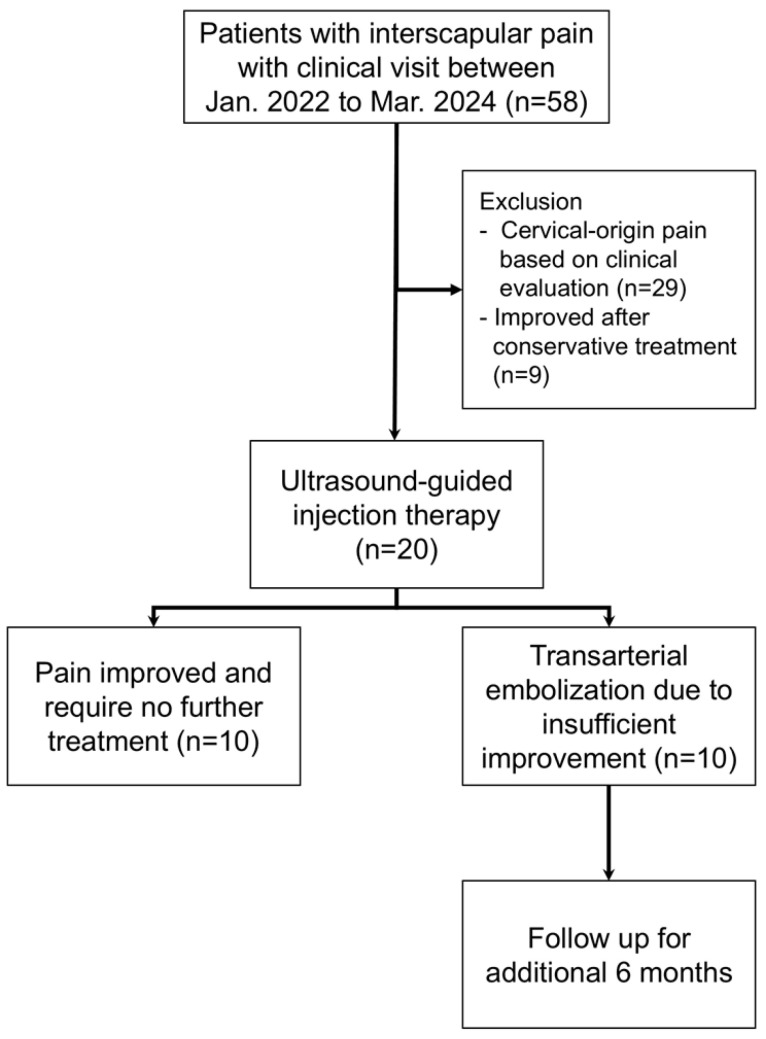
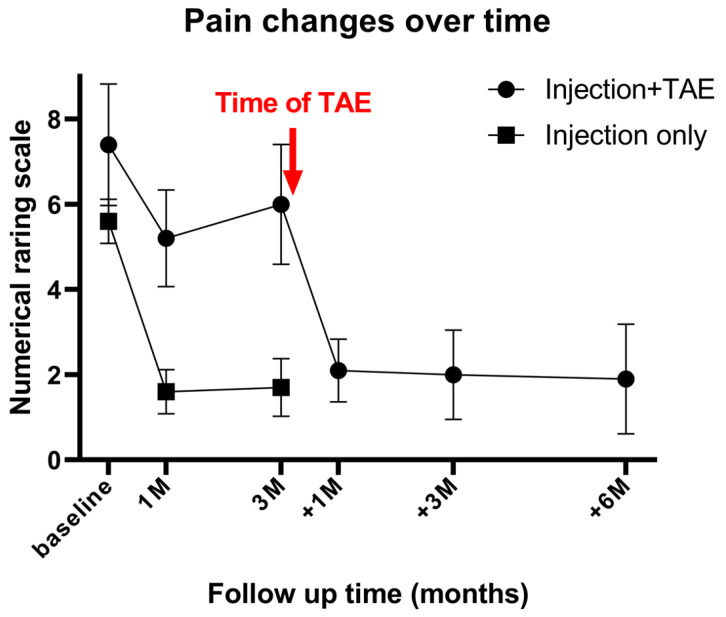
Objective: Chronic non-cervical-origin interscapular pain remains challenging to treat when refractory to conservative management and ultrasound-guided injections. This retrospective feasibility study aimed to assess the feasibility, procedural practicality, safety, and preliminary clinical outcomes of transarterial embolization (TAE) as a salvage therapy in this patient population. Methods: This single-center retrospective study included 20 patients with chronic interscapular pain (Numeric Rating Scale [NRS] score ≥5 for >3 months) who initially underwent ultrasound-guided injection therapy. Patients who experienced inadequate pain relief after 3 months (n = 10) proceeded to TAE, while the remaining 10 patients with sufficient relief formed the comparison group. TAE primarily targeted the transverse cervical artery using imipenem/cilastatin sodium as the embolic agent. Pain outcomes were assessed using NRS scores at 1, 3, and 6 months post-procedure. The primary outcome was pain reduction (≥50% decrease in NRS score), with secondary outcomes including technical success, medication use, and safety assessment. Results: The mean baseline NRS score for all patients was 6.5 ± 1.4, which decreased to 3.4 ± 2.0 at 1 month and 3.9 ± 2.5 at 3 months post-injection (p < 0.001). In the TAE group, the NRS score decreased from 7.4 ± 1.4 to 5.1 ± 1.1 at 1 month and 6.0 ± 1.4 at 3 months, indicating inadequate pain relief. In contrast, the injection-only group showed significant improvement, with NRS scores decreasing from 5.6 ± 0.5 to 1.6 ± 0.5 at 1 month and 1.7 ± 0.7 at 3 months (p < 0.001). The reduction in NRS scores was significantly less in the TAE group compared with the injection-only group (-2.2 vs. -4.0 and -28.7% vs. -71.4% at 1 month; -1.4 vs. -3.9 and -18.2% vs. -69.7% at 3 months; all p ≤ 0.001). Following TAE, the mean NRS score further decreased to 2.1 ± 0.7, 2.0 ± 1.1, and 1.9 ± 1.2 at 1, 3, and 6 months, respectively (p < 0.001), with clinical success rates of 90%, 100%, and 90% at these respective time points. At the final follow-up, the percentage of NRS score reduction was comparable between the TAE and injection-only groups (-74.8% vs. -69.7%, p = 0.397). No severe or life-threatening adverse events were observed; only self-limited adverse events were reported. Conclusions: In this retrospective feasibility study, TAE appeared safe and effective as a salvage therapy for patients with refractory non-cervical-origin interscapular pain unresponsive to injection therapy. Further prospective, randomized studies are needed to validate these findings, refine patient selection criteria, and optimize treatment outcomes.
目的:慢性非颈源性肩胛间疼痛在保守治疗和超声引导下注射治疗难治性时仍然具有挑战性。这项回顾性可行性研究旨在评估经动脉栓塞(TAE)作为一种挽救性治疗在该患者群体中的可行性、程序实用性、安全性和初步临床结果。方法:本单中心回顾性研究纳入20例慢性肩胛间疼痛患者(数值评定量表[NRS]评分≥5,持续bbbb3个月),最初接受超声引导注射治疗。3个月后疼痛缓解不足的患者(n = 10)进行TAE,其余10例缓解充分的患者作为对照组。TAE主要针对颈横动脉,使用亚胺培南/西司他汀钠作为栓塞剂。术后1、3、6个月采用NRS评分评估疼痛结局。主要结局是疼痛减轻(NRS评分下降≥50%),次要结局包括技术成功、药物使用和安全性评估。结果:所有患者的平均基线NRS评分为6.5±1.4,注射后1个月降至3.4±2.0,3个月降至3.9±2.5 (p < 0.001)。TAE组的NRS评分从1个月时的7.4±1.4下降到5.1±1.1,3个月时的6.0±1.4,表明疼痛缓解不足。单纯注射组的NRS评分从1个月时的5.6±0.5降至1.6±0.5,3个月时的1.7±0.7 (p < 0.001)。与单纯注射组相比,TAE组NRS评分的降低明显更小(1个月时-2.2 vs -4.0, -28.7% vs -71.4%; 3个月时-1.4 vs -3.9, -18.2% vs -69.7%,均p≤0.001)。TAE后,平均NRS评分在1、3和6个月分别降至2.1±0.7、2.0±1.1和1.9±1.2 (p < 0.001),临床成功率分别为90%、100%和90%。在最后随访时,TAE组和单纯注射组的NRS评分降低百分比相当(-74.8% vs -69.7%, p = 0.397)。未观察到严重或危及生命的不良事件;仅报告了自限性不良事件。结论:在这项回顾性可行性研究中,TAE作为一种对注射治疗无反应的难治性非颈源性肩胛间疼痛患者的挽救性治疗是安全有效的。需要进一步的前瞻性随机研究来验证这些发现,完善患者选择标准,优化治疗结果。
DiagnosticsBiochemistry, Genetics and Molecular Biology-Clinical Biochemistry
CiteScore
4.70
自引率
8.30%
发文量
2699
审稿时长
19.64 days
期刊介绍:
Diagnostics (ISSN 2075-4418) is an international scholarly open access journal on medical diagnostics. It publishes original research articles, reviews, communications and short notes on the research and development of medical diagnostics. There is no restriction on the length of the papers. Our aim is to encourage scientists to publish their experimental and theoretical research in as much detail as possible. Full experimental and/or methodological details must be provided for research articles.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


